Download
1 / 16
160 likes | 164 Views
Dialysis Modality and Incident Atrial Fibrillation in Older Patients With ESRD. Jingbo Niu , Maulin K. Shah, Jose J. Perez, Medha Airy, Sankar D. Navaneethan, Mintu P. Turakhia , Tara I. Chang and Wolfgang C. Winkelmayer 2019.04.03 Chih-Hsin , Yeh. Introduction.

E N D
Dialysis Modality and Incident Atrial Fibrillation in OlderPatients With ESRD JingboNiu, Maulin K. Shah, Jose J. Perez, Medha Airy, Sankar D. Navaneethan, Mintu P. Turakhia, Tara I. Changand Wolfgang C. Winkelmayer 2019.04.03 Chih-Hsin, Yeh
Introduction • Atrial fibrillation/flutter (AF) is the most commonsustained arrhythmia in the general population and isparticularly common in patients with end-stage renaldisease (ESRD). • More than 10% of prevalent US patientson hemodialysis (HD) therapy carry a confirmed diagnosisof AF, and the percentage increases steeply withage, reaching approximately one-quarter of patientsolder than 85 years. • The cumulative incidence of newlydiagnosed AF during the first year of dialysis therapyamong older patients initiating HD is almost 15%.
Introduction • Several risk factors for the developmentof AF have been identified, including sociodemographiccharacteristics and chronic conditions(eg, heart failure, diabetes, and hypertension), and itappears that most of these factors similarly increaseAF risk in patients with kidney failure requiring maintenancedialysis. • One potential AF risk factor unique to patients withkidney failure that has not been investigated sufficiently isthe dialysis modality used for kidney replacement therapy.
Introduction • Patients undergoing HD are exposed to considerable cyclical changes in fluid and electrolyte status with accumulation of fluid and uremic toxins, including potentially pro-arrhythmogenicelectrolytes during the intradialytic interval followed by rapid fluid removal and electrolyte shifts during the relatively short HD procedure. • By contrast, PD confers more continuous removal of excess fluids and maintenance of electrolyte balance, thus exercising less strain on the heart while reducing the burden of other potential AF triggers.
Objective • However, little is known about whether the AF incidence differs between patients undergoing HD versus PD. • We conducted this study to specifically challenge the null hypothesis of no difference in AF incidence between incident patients with ESRD using PD versus HD in a large ESRD registry.
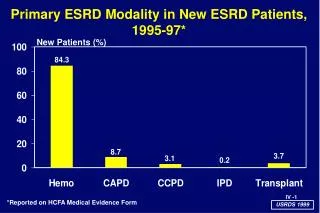
Methods Study Design:Retrospective cohort study. Source Population : Using the US Renal DataSystem, we identified older patients (≥67 years)with Medicare Parts A and B who initiated dialysistherapy (1996-2011) without a diagnosis of AFduring the prior 2 years.
Methods Exposure: Dialysis modality at incident end-stagerenal disease (ESRD) and maintained for at least90 days. We excluded patients who died on the index date or underwent preemptive kidney transplantation, discontinued dialysis therapy, recovered kidney function, or were lost to follow-up during the 90 days following the index date. Outcome: Patients were followed up for 36months or less for a new diagnosis of AF.
Methods Statistical Analysis Time-to-event analysisusing multivariable Cox proportional hazardsregression to estimate cause-specific HRswhile censoring at modality switch, kidneytransplantation, or death. Then weapplied the Fine-Gray model to estimate the subdistributionHR. This model considered persons withcompeting events as being still in the risk set whendefining the hazard of AF and is preferable in “predictingan individual’s risk.”
Discussion • Why thebenefit of PD for AF risk is not sustained is unclear. Perhapsit is related to the complex pathophysiology of AF. • Becausepatients with kidney failure have volume overload long term and neurohormonal alterations leading to cardiacstructural abnormalities, modality differences for dialysismay not be enough to reduce the risk for AF. • It has beenshown that chronic inflammation and oxidative stress maybe implicated in the pathophysiology of AF, both of whichare present in patients with kidney failure on any dialysismodality.
Discussion Limitations: • Residual confounding from unobserveddifferences between exposure groups; • ascertainment of AF from billing claims; • study offirst modality may not generalize to patientsswitching modalities; • uncertain generalizability toyounger patients.
Conclusion • Although patients initiating dialysistherapy using peritoneal dialysis had a lower AFincidence during the first 90 days of ESRD,there was no major difference in AF incidencethereafter. • The value of interventions to reducethe early excess AF risk in patients receivinghemodialysis may warrant further study.