Download
1 / 18
190 likes | 375 Views
Unstable angina and arterial hypertension. Leszek Kinasz, MD American Heart of Poland Ustron, Poland. Clinical data. Female, 59 years old Unstable angina (CCS class 4) Hypertension since 1999, currently required 4 drugs (ACEI, beta-blocker, duretic, calcium channel blocker)

E N D
Unstable angina and arterial hypertension Leszek Kinasz, MD American Heart of Poland Ustron, Poland
Clinical data • Female, 59 years old • Unstable angina (CCS class 4) • Hypertension since 1999, currently required 4 drugs (ACEI, beta-blocker, duretic, calcium channel blocker) • Hypercholesterolaemia • History of pulmonary oedema • BMI 35
Clinical data • RR 220/120 • HR 64/min • Pulmonary congestion • EKG: ST depression and negative T wave in inferior and lateral leads • UKG: LVEF 55%, hypokinesia of inferior segments, MVI(+) • Lab tests: CPK, CPK-MB, Troponin I - normal, Creatinine 1.4 mg%
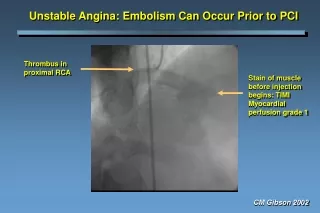
Coronary angiography (CAG) LCA RAO30, Caud 15 Normal epicardial segments RCA LAO60:99% lesion in distal segmenttype B2
PCI: 7F JR guiding cath, 0,014” BMW wire, RCA LAO60:predilatation and stent positioning (BX Velocity 3.0x18 mm) After stenting: max. pressure 18atm
After PCI: • Persisted chest pain and ST/T changes on the EKG monitor • RR 200/120 -a rigorous treatment of hypertension(NTG i.v. and i.a., Furosemid i.v., nifedipine s.l.) without effect on angina
What is a cause of the chest pain? • Occlusion of a small AM branch? AM
What is a cause of the chest pain? • Hypertension?If so, what should be done next?1. More intensive pharmacological treatment2. Further diagnosis of hypertension
Renal angiography Right renal artery Left renal artery Angio performed in AP view, with Right Judkins catheter used previously for PCI
Renal stenting as a one-stage procedure with PCI: Renal stenting:Guiding catheter: 7F, Judkins RightWire: 0,014” BMW Stent: Corinthian 6.0mm, 14 atm, Left renal artery after stenting
Diagnostic cath, PCI and Renal Stenting as one-stage procedure: • Coronary diagnostic catheters: 2 • No of wires: 1 • No of guiding catheters: 1 • No of balloon catheters: 1 • No of stents: 2 • Contrast: Ultravist 190 ml • X-Ray exposition 10.5 min.
After the procedure • No chest pain • Arterial pressure: 150/90 • Resolution of ST/T changes in serial ECG • Lab tests on the next day:-cardiac enzymes in normal range-serum creatinine 1.2 mg% • Hospital stay: 36 hours
Discussion: • Symptoms suggesting renal artery stenosis (RAS)in the presented patient: • -short history of hypertension-diastolic hypertension resisted to pharmacological treatment-the history of pulmonary oedema despite of preserved global LVEF
CAD & RAS • In 15% of patients undergoing CAG, a significant RAS (>50%) can be foundNo of narrowed Riskcoronary arteries of RAS0 8.8%1 10.7%2 17.6%3 29,9%LM 39.0% (The Duke University Experience)
AMI Revascularization(PTCA or CABG) No-RAS RAS p 13.8% 41% 0.01 33.1% 58.3% 0.01 RAS & Risk of MACE (The Duke University Experience)
The influence of renal stenting on UA and CHF N=48 pts with UA or CHF and concomitant uni- or bilateral RAS Results: After renal stenting resolution of symptoms in 88% of patients during 8.4 months follow-up. Am J Cardiol 1997;80:363-6
Influence of renal stenting on renal function months Circulation 1998;98:642-7
Conclusions: • Patients with angina and the history suggesting RAS, coronary angiography should be always followed by renal artery angiography. • Renal artery angiography and renal stenting can be performed easily during CAG or PCI as a one stage procedure at the low risk and low additional cost.