Download
1 / 27
290 likes | 616 Views
Ultrasound appearance of nerves & needling techniques. Rafael Blanco Edinburgh Sept 2006. Portable Sonosite machines. General principles of ultrasound guided techniques (1). Select probe Set machine to musculoskeletal (small parts- SmP) or vascular (Vas) setting

E N D
Ultrasound appearance of nerves &needling techniques Rafael Blanco Edinburgh Sept 2006
General principles of ultrasound guided techniques (1) • Select probe • Set machine to musculoskeletal (small parts- SmP) or vascular (Vas) setting • Set resolution to General (Gen) • Apply layer of gel to probe or skin - place probe over target area • Orientate probe to reflect hand movements-mark on probe corresponds to dot in top left of screen.
General principles of ultrasound guided techniques(2) • Adjust depth so target structure/s are in the centre of field and screen • Determine the needle entry point by gently pressing on the skin, watching for tissue movement on the screen. • Infiltrate skin and subcutaneous tissues (under direct vision if necessary)- apply protective sheath to probe • Disinfect skin then apply either sterile ultrasonic gel or spray with alcohol
General principles of ultrasound guided techniques (3) • Insert needle through skin- identify needle tip (DO NOT advance unless needle tip is identified) • Direct needle to lie next to (do not touch) target nerve • Inject 2mls - local anaesthetic - watch spread (enclircling nerve), reposition if necessary REMEMBER: NEVER advance the needle blindly, ALWAYS remove air from the injectate (white out!!)
General principles of ultrasound guided techniques (4) • PARALLELISM: The more parallel the needle to probe face - better the visibility (shallow approach) • ANISOTROPY: Maximum reflection if structure is seen at 90° to probe (range 45 - 90°) • Needle (design / coating)-- no evidence that needle design improves needle visibility • Doppler or Colour pulsed Doppler is essential for distinguishing vessels from nerves and observing flow characteristics
Frequency: 5-10 MHz Maximum Depth: 7 cm Maximum Field of View: 38 mm High Spatial Resolution ~ 0.5 mm Frequency: 2-5 MHz Maximum Depth: 22 cm Lower Spatial Resolution ~ 2mm Intra-operative Superficial vascular
Probe covers • Advantages • Protect the probe from contamination (keep it clean) • Improves sterility • Disadvantages • Degrades the picture • Interfers with grip
Do nerves look the same? in part determined by: • Where it is visualised - interscalene / axilla • The surrounding tissues (they compress and shape the nerve) • The amount of connective tissue in the nerve determines the appearance of the nerve (echogenicity) • interscalene - black holes (pure nerve - little connective tissue) • peripheral nerves - speckled - bright (lots of connective tissue - increasing durability
But also… • Size of the nerve • Depth from the skin • Probe design (linear or curvilinear) Frequency of beam (MHz) • Angle of incidence of beam – structures best seen at 90° to beam (reduce anisotropic effect)
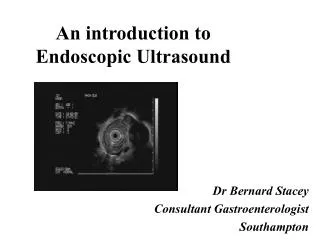
Longitudinal view Each nerve appears as a relatively hyper echoic band characterized by multiple discontinuous hypo echoic stripes separated by hyper echoic lines. As the fascicles are the main sonographic feature of peripheral nerves, their appearance has been described as a ‘fascicular pattern’,
Line Placement Across Longitudinal
So… conceptually easier to do shortest distance to nerve mimics original approaches • position confirmed by injection of solution • less painful • after introduction of needle – may need to angle the probe to find the needle
Along the long axis of the probe (parallel to the probe) – the needle can be visualised throughout its entire length • The closer the needle is to being parallel the better the picture • Difficult to keep needle directly under the beam (beam width 1mm) • More discomfort – passing through muscle
Insertion angle and visibilitySchafhalter-Zoppoth et al: RAPM Sept-Oct 2004
Needle gauge and visibilitySchafhalter-Zoppoth et al: RAPM Sept-Oct 2004
Varying needles seen at 0º& 45 ºSchafhalter-Zoppoth et al: RAPM Sept-Oct 2004 18G - Hustead epidural needle 18G - UP Tuohy needle 18G - Standard Sprotte (pencil tip) needle 18G - Spinal (Quincke tip) needle
Needling, general principles • Choose an approach that you are familiar with • Know the anatomy of the area of interest • Choose the probe suitable both for access and depth • Identify a reference structure - for orientation - pattern recognition
Practical application • Identify relevant nerve - scan proximally / distally, change angle of probe - to obtain best picture. • Make sure you can hold a stable image - change from dominant to non dominant hand. • Identify entry point - avoiding overlying vascular structures • Avoid inserting needles through muscles and flexor surface of forearm.
Golden rules • Always move the probe to find the needle - don’t look for the probe with the needle • Never advance the needle unless you identify or visualize the needle tip • Do not impale the nerve - place the needle beside the nerve
Artefacts • Acoustic shadowing • Air • Post cystic enhancement • Needle reverberation • Anisotropy