Download

1 / 51
520 likes | 530 Views
Reducing Length of Stay The Guildford Experience. Iain Jourdan Consultant surgeon and Senior Tutor Minimal Access Therapy Training Unit. Lancet. 1995 Mar 25;345(8952):763-4. Recovery after laparoscopic colonic surgery with epidural analgesia, and early oral nutrition and mobilisation.

E N D
Reducing Length of Stay The Guildford Experience Iain Jourdan Consultant surgeon and Senior Tutor Minimal Access Therapy Training Unit
Lancet. 1995 Mar 25;345(8952):763-4. Recovery after laparoscopic colonic surgery with epidural analgesia, and early oral nutrition and mobilisation. Bardram L, Funch-Jensen P, Jensen P, Crawford ME, Kehlet H. Department of Gastrointestinal Surgery, Hvidovre University Hospital, Copenhagen, Denmark. Professor Henrik Kehlet
Elements of enhanced recovery PRE-ADMISSION COUNSELLING managing expectations preparing for in-patient programme training for home care
Elements of enhanced recovery NO MECHANICAL BOWEL PREP Reduced risk of dehydration and electrolyte imbalance No greater risk of anastomotic leak or mortality
Elements of enhanced recovery CARBOHYDRATE LOADING Reduced starvation period more acceptable to pt Insulin resistance reduced/improved nitrogen balance One RCT claiming a reduction of 3 days in-pt stay with CHO loading!
Elements of enhanced recovery ANAESTHETIC PRACTICE Short acting agents No premed Regional anaesthesia
Elements of enhanced recovery FLUID MANAGEMENT Not too much - not too little Goal directed
Fluid management Morbidity Fluid Load Bellamy MC. BJA 2006;97:755-7
Doppler guided fluid optimisation Measure stroke volume 10% fall in stroke volume 250mls of gelofusin over 2 min no Yes Measure stroke volume every 10 min Increase in stroke volume is greater than 10% no
Physiology - pneumoperitoneum and steep Trendelenburg • Cumulative increase SVRI (systemic vascular resistance index) • Decrease in mean cardiac index from 3.3 to 2.8 L/min/m2 • MAP initially increases from 74 to 90 mmHg • SVRI progressively decreases • MAP ultimately collapses requiring vasoconstrictors in 70% of patients (phenylephrine) • Average time to vasoconstrictor support 25 mins (5-40)
Intra-operative volume requirement Intra-operative fluid volume in first 440 patients (preERP) Minimum 800 Maximum 4200 Mean 1729 mls Std. Deviation 642.24 Intra-operative fluid volume in study group using oesophageal doppler Minimum 350 Maximum 1600 Mean 875 mls Std. Deviation 318.03
Elements of enhanced recovery PAIN CONTROL Minimise pain, minimise sedation minimal opiates regional blocks short incisions
Randomised trial - Spinal versus Epidural versus PCA(In fluid optimised patients undergoing lap colorectal resection) p=0.002 p<0.001 π δ
Advantages of spinal anaesthesia Higher insertion rate, lower complication rate Does not suffer from unilaterality, falling out, kinked tubing Far less labour intensive Wears off, patients not limited the following morning
Elements of enhanced recovery MINIMISE PHYSIOLOGICAL DISTURBANCE Maintain temperature Short operation Minimal Access Surgery No NG, catheters out early Eat and drink early
An important role for Minimal Access Surgery • 436 consecutive patients referred for elective colorectal surgery over 4 years • 25 patients (6%) excluded due to: • obesity (BMI > 35) • large (> 10 cm) masses • Obstruction • Sigmoid volvulus • 411 patients treated laparoscopically
Pathology No of Patients Cancer 232 Diverticulosis 52 Endometriosis 50 Benign polyp 28 Crohn’s disease 28 Rectal prolapse 14 Ulcerative Colitis 10 Volvulus 6 Other 10 Colorectal pathologies
Results • Median operating time = 120 mins (90-146) • 20 conversions (5%) • Stomas • 30 (7.4%) diverting stomas • 24 (6%) permanent stomas • Median wound length = 5 cm (4-6) • Overall median hospital stay = 4 days (3-5) • With stoma = 7 days (5-10) • No stoma = 3 (2-5) • Earliest discharge following left sided resection = Day 1!
The Challenge A safe 23 hr hospital stay for colorectal resection
Entry Criteria for 23-hour stay Post op(23 hrs from start of surgery) Informed consent Colonic or high rectal procedure ASA 1 or 2 Age< 75 BMI< 28 Adequate home support Competent adult present post-op 24 hours Telephone line/mobile Home< 15 miles from Hospital Incision< 7 cm Agreement GP Uncomplicated operation Patient motivated
Patient management No bowel prep No prolonged starvation Preload No opiates
Total IV fluid • Oesophageal Doppler directed intraoperative fluid • Post-op • 1L Hartmann’s over 8 hours • 1L Hartmann’s over 12 hours • 500mls colloid if mixed venous O2 <60%
Anaesthetic Standardised GA Spinal Central line Oesophageal Doppler No NG
Discharge pack Lactulose Paracetemol Voltarol with PPI if indicated Tramadol if NSAID contraindicated Staple remover
Time frame of recovery 12:00 hrs Start of operation 15:00 hrs Cup of tea in recovery 16:00 hrs Return to ward Out of bed for >2 hours Walk on spot for 5 minutes Normal dinner 20:00 hrs Mixed venous gas. If mixed venous O2 < 60% given 500ml fluid bolus 24:00 hrs Catheter removed 06:30 hrs All lines removed Breakfast Supervised walk along corridor 11:00 hrs Discharged home
Discharge basis Consensus of patient and Medical team Pain controlled Tolerating diet Unremarkable abdominal findings Walking unaided
Results 40 consecutive patients undergoing laparoscopic colorectal resection 10 fulfill criteria (25%)
Outcome • All discharged at 23 hours post surgery • No readmissions • No complications • High patient satisfaction
Why bother ? Economics Reduce costs Increase income Patient safety Hospital acquired infection directly related to Time spent in hospital Prolonged catheterisation (IV / urinary / ng) Patient debility DVT and chest infection related to Immobility Fluid overload Analgesia Patient satisfaction
Conclusion Acheivable Accurate regime at every point Oesophageal doppler is very helpful with lower fluid volumes being administered Most appropriate post-operative analgesia appears to be spinal
A Typical Enhanced Recovery Programme Pre-op education Avoidance of bowel preparation Pre-operative carbohydrate drink Avoidance of pre-op sedatives Thoracic epidural started before skin incision Upper body air heating cover Avoidance of abdominal drains Avoidace of NGT Inta-op fluid less than 3000 mls At least 800 mls orally on day 0 At least 1 nutritional supplement on day 0 pm At least 2 nutritional supplement on day 1 Termination of iv fluids on day 1 Termination of urinary drainage on day 2 Solid food eaten on day 1 Aperient given Mobilisation on the day of surgery Mobilisation of at least 6 hours on day 1 Post-operative thoracic epidural Termination of thoracic epidural on day 2
What’s the evidence ? • 2010 • meta-analysis of 6 RCTs • 452 patients
The trials Muller S, Zalunardo MP, Hubner M, Clavien PA, Demartines N.A fast-track program reduces complications and length of hospital stay after open colonic surgery. Gastroenterology 2009;136:842–7. Serclova´ Z, Dytrych P, Marvan J, Nova´ K, Hankeova´ Z, Ryska O, et al.Fast-track in open intestinal surgery: prospective randomized study. Clin Nutr 2009;28:618–24. Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ.Randomized clinical trial of multimodal optimization and standard perioperative surgical care.Br J Surg 2003;90:1497–504. Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW. Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional postoperative care after laparotomy and intestinal resection.Dis Colon Rectum 2003;46:851–9. Gatt M, Anderson AD, Reddy BS, Hayward-Sampson P, Tring IC, MacFie J. Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection.Br J Surg 2005;92:1354–62. Khoo CK, Vickery CJ, Forsyth N, Vinall NS, Eyre-Brook IA. A prospective randomized controlled trial of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer.Ann Surg 2007;245:867–72.
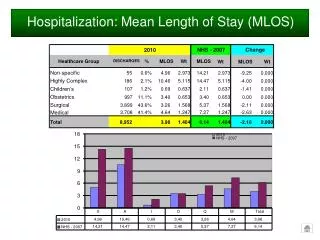
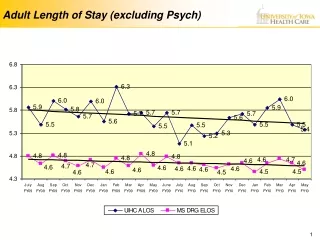
Length of stay Hospital stay reduced by over 2 days
Post operative complications Complications reduced by nearly 50%
Readmissions and mortality No difference in readmission rates or post operative mortality