Download
1 / 18
180 likes | 186 Views
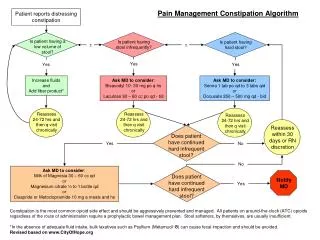
Mrs. HB visits the pharmacy seeking treatment for constipation that has developed over the past few weeks. This text provides information on the definition of constipation, risk factors, available treatment options, and factors to consider when choosing the appropriate product. It also discusses the most likely reason for Mrs. HB's acute episode and provides lifestyle advice for managing constipation.

E N D
Mrs HB comes to your pharmacy and asks to speak to you. She requests a treatment fo Constipation that has emerged over the past Few weeks. You remember that she visited your pharmacy About a month ago when she collected A new prescription for regular co-dydramol to treat her acute exacerbation of osteoarthritis of the knee.
1a What is the definition of constipation? 1b What are the main risk factors for developing constipation? 2a What risk factors for constipation apply to Mrs HB at this point in time? 2b What is the most likely reason for this acute episode? 3a What classes of drugs are available to treat constipation and how do they work? 3b Give the main indications for one drug from each group: lactulose, senna,ispaghula husk and docusate.
3c What would be your choice of agent for Mrs HB, and why? 4a You decide that senna is appropriate for short-term treatment. Which formulations are available as over-the-counter (P and GSL) medicine 5a What factors would you take into account when helping Mrs HB to choose the most appropriate product? 5b What side-effects/cautions/contraindications would you discuss with MrsHB when you supply her with the medicine? 5c What lifestyle advice would you give Mrs HB and how would you follow-up her progress
1a What is the definition of constipation? Although there is no one definition for constipation, it is usually described as infrequent defecation, which is often accompanied by straining as well as the passage of hard, uncomfortable stool.
Risk factors include: ■ immobility ■ female gender ■ increasing age low-fibre diet ■ dehydration ■ disease (e.g. Parkinson’s disease) ■ drugs (e.g. anticholinergics, opioid analgesics, many psychotropics, etc.).
2a What risk factors for constipation apply to Mrs HB at this point in time? She has immobility from osteoporosis, she is a female older person, and she is taking drugs that could cause constipation.
2b What is the most likely reason for this acute episode? The recently prescribed co-dydramol is the most likely cause as it contains an opiate, dihydrocodeine, which can cause constipation.
3a What classes of drugs are available to treat constipation and how do they work? ■ Osmotic laxatives – increase the amount of water in the large bowel (either by drawing water from the body or by retaining the water that the laxative was given with). ■ Stimulant laxatives – stimulation of smooth muscle of the gastrointestinal tract increasing intestinal motility causing muscle contraction and thus defecation. ■ Bulk-forming laxatives – increase the volume of the stool to stimulate peristalsis. ■ Stool softener laxatives – increase the amount of fluid penetrating the stool and decrease surface tension.
3b Give the main indications for one drug from each group: lactulose, senna, ispaghulahusk and docusate. Lactulose ■ Treatment of constipation. ■ Treatment of hepatic encephalopathy (portal systemic encephalopathy); hepatic coma. Senna ■ Relief of occasional constipation.
Ispaghula husk ■ For the treatment of patients requiring a high-fibre regimen: for example, for the relief of constipation, including constipation in pregnancy and the maintenance of regularity; for the management of bowel function in patients with colostomy, ileostomy, haemorrhoids, anal fissure, chronic diarrhoea associated with diverticular disease, irritable bowel syndrome and ulcerative colitis. Docusate ■ To prevent and treat chronic constipation by softening hard, dry stools in order to ease defecation and reduce straining at stool; and in the presence of haemorrhoids and anal fissure, to prevent hard, dry stools and reduce straining. ■ As an adjunct in abdominal radiological procedures.
3c What would be your choice of agent for Mrs HB, and why? A stimulant such as bisacodyl or senna because it is for occasional use. This group is also pharmacologically appropriate as they improve gut motility, which is currently reduced by the opiate in co-dydramol. Docusate can be used as it has both stimulant and softener actions. Note: As these medications may be purchased over the counter, docusate is a more expensive choice. 4a You decide that senna is appropriate for short-term treatment. Which formulations are available as over-the-counter (P and GSL) medicines? Senna is available in the form of tablets, chewable tablets, granules or liquid (oral solution).
5a What factors would you take into account when helping Mrs HB to choose the most appropriate product? Factors to take into account include: ■ palatability ■ swallowing ■ personal preference (taste, preference for specific dosage form – tablet, liquid) ■ previous experience ■ side-effects.
5b What side-effects/cautions/contraindications would you discuss with MrsHB Side-effects • Senna may cause abdominal cramps and diarrhoea. Prolonged use of sennamay produce watery diarrhoea with excessive loss of fluid and electrolytes, particularly potassium, muscular weakness and weight loss. • Changes in the intestinal musculature associated With malabsorption and dilation Of the bowel, similar to ulcerative colitis and to megacolon, may also occur. • Cardiac and renal symptoms Have been reported. • Melanosis coli and a red or yellow discoloration of the urine and faeces may also occur.
Cautions • Use should be reviewed after a week. Senna should not be used for prolonged periods since it may decrease the sensitivity of the intestinal mucous membranes, So larger doses have to be taken and the bowel fails to respond to normal stimuli. Contraindications • Mrs HB should stop taking senna if she has severe abdominal pain, feels sick or vomits. If these occur Mrs HB should see her doctor. In general, laxatives should not be taken where there is severe abdominal pain or used regularly for prolonged periods, except on medical advice. • Over-the-counter senna should not be used when abdominal pain, intestinal obstruction, nausea or vomiting is present.
5c What lifestyle advice would you give Mrs HB and how would you follow-up her progress. • Increase dietary intake of fibre, only if 1.5–2.0 L daily fluid intake is possible. • Add 30 g unprocessed bran to food or fruit juice, especially if stools are small and hard. • Encourage establishment of regular bowel habits. Explain the importance of adopting good positioning (sitting with knees above hips, feet on the floor/well supported) to facilitate bowel movement if it is possible for MrsHBto do this. • Encourage regular exercise within her ability.
Recommend that she contacts you in a few days and discusses the efficacy of the product. Discuss the need for discontinuing the senna if she no longer needs the co-dydramol. It would be worth discussing whether Mrs HB can step down her analgesia to paracetamol alone which should lead to resolution of the constipation.