Download
1 / 58
580 likes | 679 Views
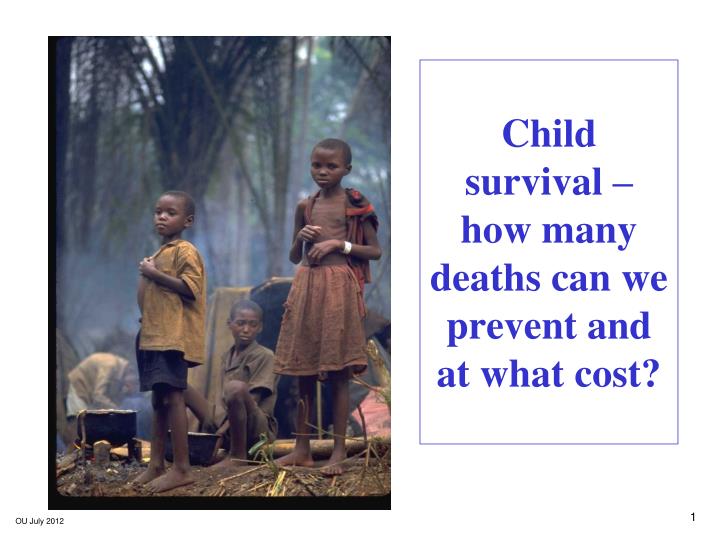
Child survival – how many deaths can we prevent and at what cost?. Child mortality and aspects to be covered. An evidence based approach to reducing under-5 deaths. Estimation of costs Actual experiences. Worldwide around 9 million children under 5 years of age are dying each year.

E N D
Childsurvival – how many deaths can we prevent and at what cost?
Child mortality and aspects to be covered • An evidence based approach to reducing under-5 deaths. • Estimation of costs • Actual experiences Worldwide around 9 million children under 5 years of age are dying each year
Mortality by cause Interventions Model Resources Impact on mortality A model for linking interventions to Impact on under-5 mortality
Mortality by cause Interventions Model Resources Impact on mortality A model for linking interventions to Impact on under-5 mortality
24 countries in which over 90% of under-5 deaths occur Neonatal division Asphyxia - 29% Sepsis - 25% Tetanus - 7% Prematurity - 24% (Other is 15%)
Mortality by cause Interventions Model Resources Impact on mortality A model for linking interventions to Impact on under-5 mortality
Intervention selection Central criterion for selection of any intervention is feasibility for delivery at high levels of population coverage in low-income countries. Each potential intervention assigned to one of three levels based on the strength of evidence for its effect on child mortality. 1 – sufficient evidence of effect 2 – limited evidence of effect 3 – Inadequate evidence of effect
Die Interventions by cause - diarrhoea Prevention Treatment Breastfeeding Exposure to diarrhoea Water/San/Hygiene Complementary feeding Oral rehydration therapy Zinc Vitamin A Diarrhoea Antibiotics for dysentry Zinc Survive Future: rotavirus vaccine
Die Interventions, neonatal - prematurity Prevention Treatment Antibiotics for premature rupture of membrane Pregnant Insecticide-treated materials* Intermittent preventive therapy Antinatal steroids Premature Newborn temperature management Survive * Indoor residual spraying may be used as an alternative
Mortality by cause Interventions Model Resources Impact on mortality A model for linking interventions to Impact on under-5 mortality
Lancet model – calculation types • For each of the 24 countries in sub-Saharan Africa, the number of under-5 deaths that could be prevented was calculated with coverage levels around the year 2000 increased to 99% except for exclusive breastfeeding, where 90% was used. The calculations divided into three types: • Exclusive and continuing breastfeeding, as this involved three levels: exclusive, partial and no breastfeeding • Complementary feeding, which utilized the underweight distribution of under-5s within a country • All other interventions.
Lancet model – calculation of deaths averted For the majority of calculations the proportionate reduction of deaths when intervention coverage is increased from the current value (pc) to target (pt) is = AfEf(pt - pc)/(1 – pcEf) where Ef is the efficacy of the interventionand Af is the fraction of deaths affected by the intervention.
Mortality by cause Interventions Model Resources Impact on mortality A model for linking interventions to Impact on under-5 mortality
Lancet model – results by intervention type • Results are calculated on the basis of the situation in the year 2000. • Under-5 deaths preventable through the universal application of the level 1 and 2 interventions were of three types – deaths preventable by: • individual intervention • specific cause • group of interventions
Mortality by cause Interventions Model Resources Impact on mortality A model for linking interventions to Impact on under-5 mortality
Costing the reduction of under-5 deaths • Costs are difficult to assess: • Commission on Macro-economics and Health estimated US$7.5 billion, but not specifically for child mortality reduction • Single disease estimates, such as HIV/AIDS, malaria and measles have been made, but little use for reduction of child mortality However, with publication of cause-of-death estimates and Lancet model on child deaths that could be averted through use of a package of effective interventions, more can be done on costing the achievement of the MDG on child survival
Source: Bryce et al, Can the world afford to save the lives of 6 million children each year? Lancet June 2005
Source: Bryce et al, Can the world afford to save the lives of 6 million children each year? Lancet June 2005
Source: Bryce et al, Can the world afford to save the lives of 6 million children each year? Lancet June 2005
Additional annual running Variable value cost (US $ millions) Variable assessed Low High Low High Country specific cost of community delivery agent relative to cost of a 50% 100% 4311 5955 midwife (originally 75%) Drug costs -25% +25% 4598 5669 Existing intervention coverage level in +25% -25% 4210 6374 year 2000 All three variables 3111 8083 Child mortality reduction: effects of varying assumptions on additional running costs Source: Bryce et al, Can the world afford to save the lives of 6 million children each year? Lancet June 2005 Individual country costs and situations differ widely
Costing assumptions Average cost per death averted about $890, with neonatal death averted at around $780. But 2005 Lancet neonatal series estimated death averted cost of $2100 (over half of this due to provision of emergency obstetric care). Estimates did not include capital, hiring, training and other infrastructure development costs. Consumer costs were not included. Vaccines and drug cost estimates do not account for expected cost reduction as demand increases However, resources linked to appropriate intervention packages are critical if money is to be effectively used to reduce child mortality
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Accelerated child survival and development (ACSD) in West Africa • 11 countries in West Africa • Support from CIDA and other partners • Aim: To reduce mortality among children less than 5 years of age • Strategy: Accelerate coverage with three packages of high-impact interventions, with a special focus on community-based delivery
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Three intervention packages • Routine EPI+ • Strengthening routine EPI • Vitamin A supplementation • IMCI+ • Family practices promotion • Exclusive breastfeeding • ORT • ITNs (pregnant and under-5s) • Community management of malaria and ARI • Antenatal care+ (ANC+): • Refocused ANC4 • Tetanus immunization • Intermittent presumptive treatment (IPT) against malaria • Vitamin A (post partum) Concept and aim: three packages covering three service delivery modes, plus strengthening local accountabilities through performance contracts and participatory monitoring Started with limited package: EPI+ & ANC+ & ITNs
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Districts • 16 “high impact”* (population ≈ 3million) • 31 “expansion” (population ≈ 14 million) *now 18 districts, because the Upper East Region of Ghana has been reorganized and now includes 8 rather than 6 districts. ACSD geographic coverage • Countries • 4“high impact” Benin, Ghana, Mali, Senegal • 7 “expansion”
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Evaluation questions Impact Were there changes in nutrition and mortality in the ACSD “high-impact” districts? Were these changes greater than in the comparison area? Attribution Is it plausible to attribute the impact found to ACSD? Coverage • Were there changes in the ACSD “high-impact” districts? • Were these changes greater than in the comparison area?
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Evaluation design • Intervention areas • ACSD “high impact” countries/districts (Benin, Ghana, Mali, Senegal) • Comparison areas • All other districts in the country, excluding major metropolitan areas
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Data sources: All existing data that met quality standards
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) ACSD Implementation • EPI+ • Immunizations and vitamin A supplementation implemented first and most strongly in all four countries • ITNs started strong, but stockouts at UNICEF-Copenhagen limited provision of new nets for >1 year at crucial time • IMCI+ • Facility component received little support • Community component started only in mid to late 2003 • Many messages, some unlikely to affect child mortality • Community tx of pneumonia not included at scale • ACTs not available at community level in any of the three countries • Interventions to address undernutrition given low priority • ANC+ • ACSD inputs focused on IPTp with SP and postnatal vitamin A
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Key Coverage for EPI+ interventionsbefore and after ACSD, in HIDs Before ACSD After ACSD Benin Ghana Mali Increases in coverage across the board in Ghana and Mali; Benin achieved increases for vitamin A and ITNs.
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Key Coverage for IMCI+ interventionsbefore and after ACSD, in HIDs Before ACSD After ACSD Benin Ghana Mali No coverage gains, and some significant losses, in sick child care. Exclusive breastfeeding increased in Ghana, declined in Mali.
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Coverage for ANC+ interventionsbefore and after ACSD, in HIDs Key Before ACSD After ACSD Benin Ghana Mali Ghana and Mali improved care for childbearing women; delivery of TT and postnatal vit A benefited from EPI system in Mali.
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Research question #1:Increases in coverage in ACSD HIDs? • Benin • Yes for ITNs and vitamin A supplementation • No for all other ACSD interventions • Ghana and Mali • Yes, especially for EPI and other interventions delivered through outreach or campaigns • No, especially for case management of diseases that cause ≈ 60% of child deaths (pneumonia, malaria, diarrhea) • Mixed results for infant feeding practices
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Research question #3: Under-five mortality in the ACSD HIDs
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Research question #4: Under-five mortality in the ACSD HIDs and national comparison areas
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Research question #5: Is it plausible to attribute the accelerated impact found to ACSD? Nutrition Mortality Benin: No impact found Ghana: Yes, for stunting,but only in period 1998 – 2003. Mali: No impact found Benin: No impact found Ghana: Unknown Mali: No impact found
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Conclusions (1) • Intervention coverage CAN be accelerated if there is adequate funding & human resources. • Acceleration of mortality declines require: • Focus on interventions that have a large and rapid impact on major causes of child death • Sufficient time to fully implement approach and for coverage to translate into declines in mortality and undernutrition • Reasonable expectations, given level of resources
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Conclusions (2) Policy barriers prevented key ACSD interventions directed at pneumonia and malaria from being fully implemented. Breakdowns in commodities and gaps in funding vitiate progress toward impact. More attention and operations research needed on incentives and supports for community-based workers
Three intervention packages Immunization “plus” (EPI + ITNs, deworming & vitamin A) ANC+ (Care for mother,TT, IPTp) IMCI+ (Improved management of pneumonia, malaria and diarrhea, and key family practices) Conclusions (3) Careful monitoring with local capacity to use results is essential. Evaluation improves programs and prospective evaluations are preferred to retrospective. A new paradigm for impact evaluations is needed, that takes into account the absence of true comparison groups (see Lancet online July 9, 2010 – Victora, Black, Boerma & Bryce) See article: Lancet vol 375 pp 572-82, Feb.13, 2010
But there have been changes since the 2003 Lancet series on child survival • Changes to: • Causes of under-5 deaths • Interventions and their efficacy • Under-5 mortality rate envelope • Model used - LiST
Lancet child survival series 2003 – paper 1, figure 5 Reference year: 2000, with 10.8 million under-5 deaths
Distribution of Causes of Child Deaths: Global Global, regional, and national causes of child mortality in 2008: a systematic analysis, Lancet 375:1969, 2010 Global (8.8 million under-5 deaths) Reference year: 2008
Distribution of Causes of Child Deaths: Sub-Saharan Africa Reference year: 2008
Distribution of Causes of Child Deaths: Southeast Asia Reference year: 2008
Major Changes in Estimation Methods in 2008 Compared with 2000-2003 • New estimates of national mortality rates in children < 5 years and in neonates • Multicause models increased datapoints (102→148) • Considerable improvement in data sources, including use of national data for India and China • Multicause model used instead of single-cause models for age-group of 1-59 months (similar to previous multicause neonatal model) • Causes of death estimated for 193 countries compared with 42 countries in 2003 Lancet paper