Download
1 / 20
200 likes | 880 Views
Lisfranc Injuries. Jennifer Derrick Radiology Period 7. Who?. Jacques Lisfranc (1790-1847) devised a new amputation technique that saved time by avoiding bones. He followed a series of joints which now is collectively called the Lisfranc joint. He did not describe the injury patterns.

E N D
Lisfranc Injuries Jennifer Derrick Radiology Period 7
Who? • Jacques Lisfranc (1790-1847) devised a new amputation technique that saved time by avoiding bones. He followed a series of joints which now is collectively called the Lisfranc joint. • He did not describe the injury patterns.
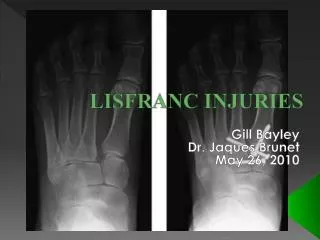
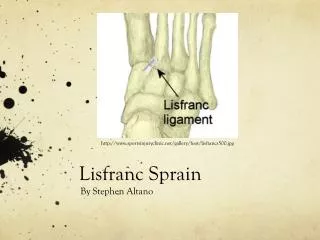
Anatomy • Tarso-metatarsal joint • Midfoot • Bones held in place by ligaments. • No ligament connection between 1st and 2nd metatarsals
Mechanism of Injury • Direct trauma/crush • Twisting • Plantar flexion with axial loading • Low or high energy (beware of associated injuries)
Clinical Presentation • Variable • Pain, especially with weight bearing activity • Plantar ecchymosis • Dorsal tenderness, edema • Mild discomfort • Deformity/instability • High index of suspicion based on mechanism!
Diagnosis • Physical exam-pronate and supinate midfoot with fixed hindfoot. • 3 view X-Ray (AP, lateral, medial oblique)-weight-bearing films helpful. • 20% of films are negative initially. Repeat films at 7-14 days, consider CT/MRI. • Often mistaken as a sprain-when in doubt, splint and refer to ortho.
Fracture/dislocation findings • The most consistent finding is misalignment along the medial side of second MT and second cuneiform.
Fracture/dislocation findings • The medial cuneiform-second MT space should be evaluated for the "fleck sign" indicating avulsion of the Lisfranc ligament.
Classification • Homolateral • All of the metatarsals are dislocated to the same side • Usually involves the 2nd through 5th dislocated laterally • Divergent • May be associated with a fracture of the 1st cuneiform • Usually involves medial displacement of the 1st metatarsal and lateral displacement of 2nd-5th metatarsals
Classification • Homolateral • All of the metatarsals are dislocated to the same side • Usually involves the 2nd through 5th dislocated laterally • Divergent • May be associated with a fracture of the 1st cuneiform • Usually involves medial displacement of the 1st metatarsal and lateral displacement of 2nd-5th metatarsals
Treatment • Depends on severity • RICE • If no dislocation--immobilize and no weight bearing for 4-8 weeks • If significant dislocation--closed reduction or ORIF
Complications • Compartment Syndrome • Chronic pain secondary to posttraumatic osteoarthritis • Repeated injuries