Download
1 / 82
1.23k likes | 5.27k Views
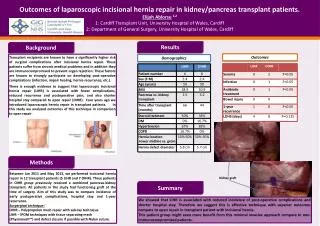
CASE PRESENTATION AND SHARING OF INFORMATION ON INCISIONAL HERNIA. by Michael Angelo L. Suñaz, M.D. Department of Surgery Ospital ng Maynila Medical Center. R.C, 58/M TONDO, MANILA. CHIEF COMPLAINT : BULGING ABDOMINAL MASS. HISTORY OF PRESENT ILLNESS:. 2 yrs PTA Px underwent ‘E’

E N D
CASE PRESENTATION AND SHARING OF INFORMATION ON INCISIONAL HERNIA by Michael Angelo L. Suñaz, M.D. Department of Surgery Ospital ng Maynila Medical Center
R.C, 58/M TONDO, MANILA
HISTORY OF PRESENT ILLNESS: • 2 yrs PTA Px underwent ‘E’ Exploratory Laparotomy, duodenorrhapy, omental patching for a Perforated PUD.
HISTORY OF PRESENT ILLNESS: • 22 months PTA noted bulging abdominal mass, about the size of the patient’s fist, most noticeable during straining or prolonged standing and reduced spontaneously when the patient assumed a recumbent position. (-) episode of vomiting (-) changes in BM
HISTORY OF PRESENT ILLNESS: • Gradual increase in the size of the abdominal mass prompted consultation and subsequent admission at the OMMC
PAST MEDICAL Hx: • s/p ‘E’ Ex-Lap, duodenorrhaphy, omental patch for Perforated Peptic Ulcer Disease – OMMC – July 2004 • No Hypertension • No DM • FAMILY Hx: No heredofamilial disease noted
PERSONAL/SOCIAL Hx: smoker, 20 pack-years, stopped last 2004 occasional alcoholic beverage drinker
PHYSICAL EXAMINATION: BP= 120/80 CR=89 RR= 20 T=36.5 HEENT: pink palpebral cojunctiva,anicteric sclera, No NAD, No CLAD, No TPC C/L: SCE, no retractions, clear BS HEART: adynamic precordium, NRRR, no murmur
ABDOMEN: Flabby, NABS, soft, non-tender (+) healed midline incision (+) mass, soft, non-tender, reducible, around the umbilicus with fascial defect approx 8 x 8 cms around the umbilicus (+) mass, soft, non-tender, reducible, 6 cms above the umbilicus with fascial defect approx 2x2 cms.
SALIENT FEATURES: • 58 y/o, M • 2-yr History of bulging abdominal mass, reducible • Fascial defect approx 8 x 8 cms and 2 x 2 cms • History of previous operation
On and off bulge at the level of the abdominal wall Abdominal wall hernia
On and off bulge at the level of the abdominal wall Abdominal wall hernia History of operation; bulge at incisional site
On and off bulge at the level of the abdominal wall Abdominal wall hernia History of operation; bulge at incisional site Incisional hernia
On and off bulge at the level of the abdominal wall Abdominal wall hernia History of operation; bulge at incisional site Incisional hernia Not reducible reducible
On and off bulge at the level of the abdominal wall Abdominal wall hernia History of operation; bulge at incisional site Incisional hernia Not reducible reducible Defect on 1 site Defect on 2 or more sites
On and off bulge at the level of the abdominal wall Abdominal wall hernia History of operation; bulge at incisional site Incisional hernia Not reducible reducible Defect on 1 site Defect on 2 or more sites strangulated Not strangulated
BASIS: Patient with history of : on and off bulging mass on incision site, s/p ‘E’ Exploratory Laparotomy without any vomiting or BM changes
TREATMENT • PRETREATMENT DIAGNOSIS: Incisional Hernia without obstruction or gangrene s/p ‘E’ Ex-Lap – July 2004
TREATMENT • GOALS OF TREATMENT: - reduce hernial content - repair the fascial defect - prevent recurrence of incisional hernia after the repair
TREATMENT OF CHOICE SUBLAY PROSTHESIS REPAIR
PREOPERATIVE PREPARATION • Informed consent • Psychosocial support • Optimize patient’s health • Screen for any condition that will interfere with treatment • Prepare materials
OPERATIVE TECHNIQUE • Patient supine under CLEA • Asepsis/Antisepsis • Sterile drapes • Excision of scarred incision skin • Subfascial flap dissection separating rectus from peritoneum/hernial sac • Hernial sac opened
OPERATIVE TECHNIQUE cont.. • Inspection of intraabdominal organs for gut adhesions and additional fascial defects • Silk suture laid on peritoneum for mesh anchoring • Interrupted Silk 2-0 sutures approximating small superior fascial defect • Excess peritoneum trimmed • Closure of peritoneum with chromic 3-0 simple continuous
OPERATIVE TECHNIQUE cont.. • Mesh laid over the area of larger defect • Anchoring sutures tied • Closure of fascia with simple continuous suture, Vicryl-0 • Hemostasis • Running continuous with Vicryl 2-0 subcutaneous • Subcuticular Vicryl 4-0 • Correct sponge, instrument and needle count • Dry Sterile Dressing
OPERATIVE FINDINGS • 7 cms fascial defect from umbilicus down and 1 cm above • Small fascial defect approx 1x1 cms, 6 cms superior to the umbilicus, left of the midline • No incarcerated bowel noted
OPERATION DONE: Incisional Herniorrhaphy with subfascial prosthesis
POST-OP CARE • Sufficient analgesia • Nutrition • Wound care • Monitoring of complications and treat as indicated • Advice on home care of wound
POST-OP CARE • Advice on ff-up plans • Avoid straining • Avoid lifting heavy objects/ learn the proper mechanics of lifting • High fiber diet • Quit smoking • Maintain a healthy weight
INCISIONAL HERNIA • occur as a complication of previous surgery • Causes: 1. poor surgical technique 2. rough handling of tissues 3. use of rapidly degraded absorbable suture materials 4. closure of the abdomen under tension, 5. infection
6. Male sex 7. advanced age 8. morbid obesity 9.abdominal distention 10. cigarette smoking 11. pulmonary disease 12. hypoalbuminemia
The incidence of incisional hernia was significantly lower when nonabsorbable sutures were used in a continuous closure; however,
the incidence of suture sinus formation (9%) and that of wound pain were significantly higher
The best definition: any abdominal wall gap, with or without a bulge, that is perceptible on clinical examination or imaging by 1 year after the index operation.
Incidence: 3 – 20% (double if the index operation is associated with infection)
Risk: midline - 10.5% transverse - 7.5%, paramedian - 2.5%
Incarceration and strangulation occur with significant frequency, and recurrence rates after operative repair approach 50%.
Classification of incisional hernias I. According to localization (modified Chevrel) • Vertical • 1.1. Midline above or below umbilicus • 1.2. Midline including umbilicus right or left • 1.3. Paramedian right or left • Transversal • 2.1. Above or below umbilicus right or left • 2.2. Crossed midline or not