Download
1 / 67
670 likes | 921 Views
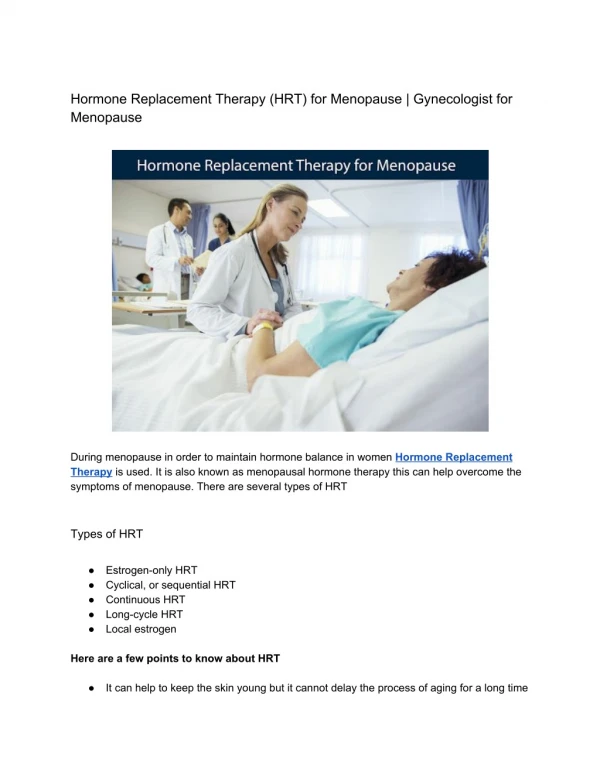
Menopause and HRT Dr. Huda Muhaddien Muhammad MBCHB ,FICOG, CABOG. Menopause refers to final menstrual period (from the Greek meno –month- ,– pausos - ending ) . Represents a watershed in the reproductive life of a women .

E N D
Menopause and HRT Dr. Huda Muhaddien Muhammad MBCHB ,FICOG, CABOG
Menopause refers to final menstrual period (from the Greek meno –month- ,–pausos- ending ) . Represents a watershed in the reproductive life of a women . The average age of the menopause in the western women is approximately 52 years.
Climacteric (from the Greek klimakter –rung of ladder-) : Signifies a major movement on life’s ladder. Is often used synonymously with (perimenopause or the changes). Is transition from the reproductive to non reproductive state.
Occurs as a result of loss of ovarian follicular activity leading to a fall in E2level below the level needed for endometrial stimulation. It can only be said to have 12 consecutive months of amenorrhea . Can occurs suddenly .
For most of the women there is gradual changes in the menstrual pattern in the years preceding the menopause as the ovarian activity fluctuates , which may be accompanied by troublesome symptoms; this is often called the perimenopause
Surgical menopause: occurs when functioning ovaries are removed as in TAH &BSO for malignancy or severe endometriosis. Iatrogenic menopause induced by treatment as radio-chemotherapy or using GnRh analogues for a variety of conditions .
Premature menopause : occurs if the menopause happens before the age of 45 . 1% of women under 40 years , 0.1 % under 30 years . It is one of the more common causes of the primary and secondary amenorrhea . the cause is usually unknown .
Well established causes of POF should be excluded:- Primary causes: Chromosomal disorders as Turner’s fragile X . 2) Auto -immune disease as hypothyroidism, Addison’s, myasthenia gravis. 3) Enzyme deficiencies as galactosaemia ,17 α- hydroxylasedefiniecy.
Secondary causes: 1) Surgical menopause after bilateral oophorectomy . 2) Chemotherapy or radiotherapy. 3) Infections like TB , mumps, malaria, varicella.
Pathophysiology: As the ovary ages the remaining follicles ( least sensitive to gonadotrophins) are increasingly less likely to mature. Ovulation declines and ovarian function gradually declines. The 1st endocrine change is a fall in Inhibin production by the ovary ( a glycoprotein that inhibits production of FSH ).
Eventually the level of estradiol production is no longer sufficient to stimulate endometrial proliferation and menopause ensues. Further decline in estradiol levels over subsequent years has effects on all estrogen –responsive tissues.
Menopause may only be a single event .but is represents a significant change in hormonal milieu and affects her future health and quality of life. Investigations : In most cases the diagnosis is pretty straightforward and doesn’t require any further investigation
It is mandatory to investigate women suspected of undergoing premature menopause. • What investigations: • FSH ( a level > 30 IU/L is considered diagnostic of menopause). • There is no value of measurement of E2, progesterone ,testostosterone in the diagnosis of the menopause. • T4 & TSH should be checked if there clinical suspention
Further assessment for screening for significant diseases in late years and introduce appropriate preventive measures: Breast screening and mammography. Endometrial assessment for abnormal bleeding. CV disease risk assessment. Skeletal assessment including bone density estimation and fracture risk assessment
Effects of the menopause : women’s experiences will vary enormously , some women have no symptoms at all; while others can have a dreadful time with debilitating symptoms that stop them functioning properly. The effects vary chronologically and are categorized as following
a/ Short term (0-5 years): • Vasomotor symptoms e.g. hot flushes ,night sweats. • Psychological symptoms e.g. labile mood ,anxiety and tearfulness . • Loss of concentration ,poor memory. • Joint aches and pains. • Dry & itchy skin. • Hair changes. • Decreased sexual desire.
b/ intermediate (3-10 years): • Vaginal dryness, soreness. • Dyspareunia. • Sensory urgency. • Recurrent UTIs. • Urogenitalprolapse. • c/ long term ( >10 years ): • Osteaporosis. • Cardiovascular disease . • Dementia.
Genitourinary problems : Urogeniotal atrophy is common observational in postmenopausal women which increases with age. Vaginal atrophy results in loss of the normal architecture within the vaginal epithelium, reducing its secretions and elasticity and making it more prone to trauma, dryness, spontaneous bleeding and infection.
Clinically this manifests as vaginal dryness, Itching, dyspareunia , vaginal pains, bleedings, discharges , and infections . Distal urethra and trigone of the bladdor are also prone to atrophy as a result of estrogens deficiency .
This can lead to urethral syndromes ( urinary frequency and dysuria in the absence of infection) , this is respond well to local vaginal estrogen. Thinning of the trigon and urethral mucosa lead to a more sensitive and trauma prone bladder which in turn leads to sensory urgency and recurrent UTI . Also this will respond to local estrogen.
Loss of estrogen plays a role in more widespread pelvic floor dysfunction leading to weakening of the supporting tissues and ligaments ( already had been damaged by childbirth) thus increase the incidence of prolapse and stress urinary incontinence .
Long term effects: • These conditions often develop without obvious clinical manifestation in the early post menopause , but pose a significant economic burden for future particularly with an increasingly ageing population. • Those women underwent premature menopause will spent a prolonged period without estregens so they are at high risk .
Osteoporpsis : Is defined as a skeletal disorders characterized by compromised bone strength predisposing to an increased risk of fracture . 20 % of our bone is composed from trabecular bone ( shock absorbing capacity)
Oestrogen acts an antiresorptive agent on the trabecular bone so E2 deficiency after menopause is characterized by unprecedented fall in bone density which ultimately may lead to increase risk of osteoporotic fractures • Bone strength is a reflection of bone quality and density .
Current strategies of treatment target preventive treatment at individual identified as high risk of subsequent fracture . • Recent NICE guidance favours a very limited role for preventive treatment for women under 75 years unless if there was history of previous fracture .
Cardiovascular disease : • Is relatively uncommon before menopause . • Oestrogen has a productive influence against CHD. • Early menopause without estrogens is associated with 2-4 increased fold of CHD. • Menopause is associated with adverse metabolic changes (raise in LDL and cholestrol and fall in HDL).
Loss of oestrgen lead to vasoconstriction and atherogenesis. • Dementia is much more common among women , but the evidence for a role of estrogen and menopause in the pathophysiology of cognitive decline and dementia is conflecting.
Management the menopause is natural event and for many women there is no need to manage it at all. Awareness of the long term implications, such as osteoporosis and CV disease should be part of good preventative medicine.
The menopause consultation : History : Concentrate on ascertaining the frequency and severity of menopausal symptoms and their impact on day to day activities. Enquiry into any sexual problems , in particular vaginal dryness soreness, and bladder symptoms should be recorded
Family and personal history should focus on risk factors for CV disease , osteoporosis ,breast cancer ,thrombosis and ovarian cancer. • Any previous treatment and S/E should be noted . • Explanation the potential s/E of all teatments
Physical examination : • Abdominal examination . • Breast examination . • Cervical smear. • Bimanual assessment of the uterine size. • Assessment of the vagina for any atrophy, prolapse or incontinence.
Lifestyle : • The menopause could be an ideal time to look at changes in diet and exercise and build for a healthy future to maximize health potential . • Smoking cessation , eating sensibly and avoid extra weight . • Regular physical activity
Alternative and complementary therapies: There is little evidence for the safety and efficacy of most of them. as in the following; 1-Non prescriptive treatment Lifestyle changes (diet and exercise). Complementary therapies : acupuncture, reflexology and magnetism.
Herbal remedies : black cohosh (actaearacemosa), dong quai ( angelica sinensis ), evening primose oil , gingkp , ginseng, stjonn’swort ( hypericumperforatum). Bio- identical hormones : natural progesterone gel , DHEA , phytoestrogens ( isoflavones, red clover ).
Prescription: α-adrenergic agonist as clonodine. Beta blockers as propranolol Selective serotonin reuptake inhibitors: venlafaxine, fluoxetine, paroxitin ,citalopram .gabapentin HRT : estrogen alone, oestrogen and progestogencombintion , progestogenalon
SSRI used for hot flushes in short trials ,only used for those who cannot take HRT. For osteoporosis , the bisphosphonates are the principle of drug used . Alternative include strontium and raloxofene ( type of SERM). Those drugs have significant S/E and should be used for women over 60 year. Para thyroid hormone is reserved for women with very high risk.
Hormone replacement therapy: • Is the principle treatment available for troublesome menopausal symptoms. • Acts by replacing the hormones that are normally produced by the human ovary at physiological levels.
Oestrogen is the main hormone and is either given alone or in combination with progestogen , which should be given for all non hysteroctemised women. • Testosterone can also be given in conjuction with oestrogen. • Most HRT treatment come in combination.
Oestrogen : There are different types of oestrogen available. 1-oestradiol ( transdermal, gel ,implant). 2-oestradiolvalerate. 3-conjucated equine oestrogens. 4-oesteronesulphate. 5-oesteriol ( vaginal only).
Can be given by different doses and by different routes. • The lowest dose should be used. • Non –oral route ( especially transdermal )avoid the 1st pass effect, and are considered more physiological as they release oestradiol to the circulation, rather than oesteron.
Avoiding thr 1st pass effect reduces the impact on various metabolic parameters, such as haemostatic and coagulation system , so seems a better option in women with personal or family history of VTE or known liver abnormalities.
Non oral routes are expensive , there can be logiicalproblemaadministeratingprogestogen component simultanously . • Subcutaneous implants is reserved for those women who hysteroctemised with removal of both ovaries , ( repeated every six months). • Implants also allow the addition of testosterone.
Progesterone: • In HRT , progetogens ( synthetic progeterone) are added for at least 10 days /calender month to mimic menstrual cycle . • This will reduce the risk of endometrial hyperplasia and cancer associated with prolonged use and unopposed oestrogen.
It can be given either cyclically mimickining a natural 28 day cycle -28 days result in withdrawal bleeding ( used for perimenopausal women; Or it can be given continuously to prevent any bleeding –so called no bleed _ treatment ( used for post menopausal women)
Types of progetogens used in HRT : C -19 nor testosterone derivatives : norethisterine ( transdermal ) levonogesterel (transdermal, intrauterine). C-21 progesterone derivatives : dydrogesterone, medroxyprogesterone acetate , cyproterone acetate .
C -17 derivatives : drospirenone . Progesterone: micronized progesterone ( vaginal gel , pessary, suppository. S/E are common esp in 1st few months and can be alleviated by changing the type or the route
Levonogesterole IUD can be used in women who canot tolerate systemic progestogenes . Progestogen is not used for hystorectomized women. Testosterone : 50% from the ovaries and 50% from the fat and adrenal glands .
Menopause doesn’t affect testosterone level but decrease SHBG level this may lead to increase the level of free testosterone . • Surgical or chemoradiation induced menopause can lead to relatively deficient testosterone. • May be presented as loss of libido, fatigue.
Risks and benefits of HRT: • Still uncertainty and controversies present about HRT use and what exactly the risks are and how relevant they are to the majority of healthy post menopausal women. • HRT • Is an extremely effective treatment for menopausal symptoms and urogenital atrophy.
is an effective treatment for osteoporosis, and appears to have beneficial effects on the cardiovascular system if it started around the menopause . • Oestrogen is effective in relieving the hot flush symptoms within 4-6 weeks.