Download
1 / 152
1.52k likes | 1.71k Views
SPOUSAL ABUSE. Goals of Lecture: Assessment & Treatment. Goals of the Class. THE STRUCTURE OF ASSESSMENT THERAPEUTIC ALLIANCE RISK ASSEMENT NEUROBIOLOGY OF VIOLENCE SYSTEMIC THEORY OF DOMESTIC VIOLENCE & ATTACHMENT THEORY UNRESOLVED TRAUMA. GOALS OF ASSESSMENT PROCESS.

E N D
SPOUSAL ABUSE Goals of Lecture: Assessment & Treatment
Goals of the Class THE STRUCTURE OF ASSESSMENT • THERAPEUTIC ALLIANCE • RISK ASSEMENT • NEUROBIOLOGY OF VIOLENCE • SYSTEMIC THEORY OF DOMESTIC VIOLENCE & ATTACHMENT THEORY • UNRESOLVED TRAUMA
GOALS OF ASSESSMENT PROCESS • WORKING TO DEVELOP THE THERAPEUTIC RELATIONSHIP • ASSESS CLIENT’S SUITABILLITY FOR TREATMENT • CLINCICAL DIAGNOSIS • ASSESS VIOLENCE & SOCIAL HISTORY • ASSESS RISK FOR FURTHER VIOLENCE • PROVIDE INTERVENTION FOR VIOLENCE CONTROL • DEVELOP ASSESSMENT-BASED TREATMENT PLAN
THERAPEUTIC ALLIANCE • THE CHALLENGE… • TO BUILD A Therapeutic Alliance WITHOUT COLLUDING WITH DANGEROUS ACTING OUT BEHAVIORS • Because so many perpetrators and victims have experienced abuse by authority figures, the process is difficult.
OBSTACLES 1. LOW MOTIVATION • INVOLUNTARY CONSUMER • SECONDARY MOTIVATION: IE. KEEP PARTNER FROM LEAVING OR TESTIFYING MOST Perpetrators. AND Victims HAVE INSECURE ATTACHMENTS>AFFECTING THE WAY THEY REGULATE ATTACHMENT. BECAUSE OF THESE DEFENSE MECHANISMS>RESULTS IN CREATING MORE EMOTIONAL DISTANCE BETWEEN SELF AND OTHER. • Perpetrators MAY PULL FOR NEGATIVE REACTIONS IN THEIR THERAPISTS.
OBSTACLES FOR THE THERAPIST • Balancing client’s needs for privacy with criminal justices needs for information • Therapists anxiety about exposure to liability working with a high risk population may compromise comfort and availability
THERAPEUTIC ALLIANCE • Client , on the one hand, elevates the therapist to a position of authority • On the other hand, client believes power and authority is shared between them • A deep sense of collaboration and participation occurs in the process • A positive attachment develops, yet this is rarely true for the perpetrator due to maladaptive defenses
ATTACHMENT • Attachment is a tie or bond that binds two people and serves a psychological and biological function across a life span. • The biological function = both physical protection and the development of neurobiological capacities in the developing brain of the infant.
Attachment • The psychological function = development of the self & an understanding of self in relationship to others. • For the adult, the biological function can be physical protection but also psychological protection. As emotional caretaking allows the adult the freedom to go out and explore their world.
ATTACHMENT • For adult partners, each person can be the caregiver and the care receiver. • Balance of these roles varies from relationship to relationship.
CHARACTERISTICS OF ATTACHMENT RELATIONSHIPS • PROXIMITY MAINTENANCE • ONE WANTS TO BE CLOSE IN PROXIMITY • ONE FEELS LOSS WHEN ONE IS AWAY • THERE MAY BE ANGER AND FRUSTRATION AT REUNION
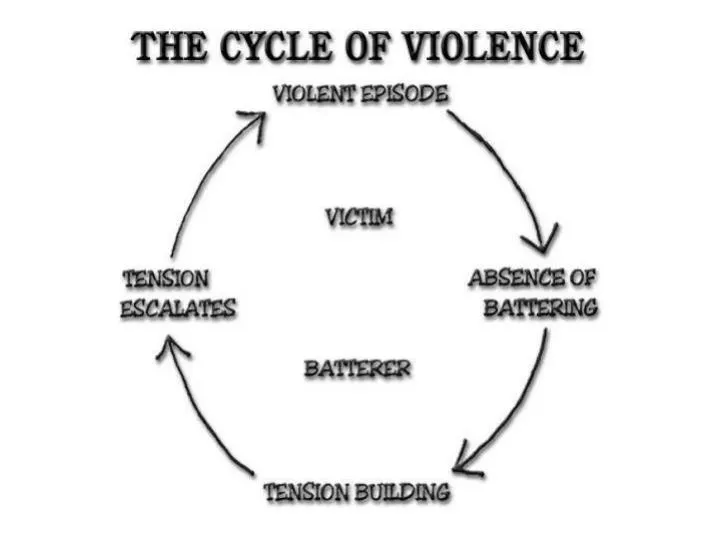
IRONIC SAFE HAVEN • ONE RETREATS TO ANGER AND FRUSTRATION WHEN FEELING ANXIOUS AND FEARFUL. • ANGER AND FRUSTRATION OFFER A SECURE BASE TO RETURN “HOME” TO.
ATTACHMENT THEORY • BOWLBY AND AINSWORTH BELIEVED THAT • SECURE ATTACHMENTS DEVELOP DUE TO • MATERNAL AND PATERNAL SENSITIVITY AND COOPERATION.
SENSITIVITY • CAREGIVERS ability to accurately interpret the infants ever changing need. To accurately read the infant and to respond accordingly within a timeliness.
4 components of sensitivity • Awareness of signals • Accurate interpretations • Appropriate response • Prompt response
COOPERATION • Do interventions break into, cut across, or interrupt the infants ongoing activity or are they geared in both timing & quality to the child’s state, mood, & current interests?
Facilitating secure attachments • Sensitivity & cooperation are the basis for healthy parent child/child interactions. • If this process breaks down the child experiences a break in the connection, or feels ignored, or intruded upon • When there is misattunement which occurs with frequency…the child becomes anxious (escalated) or cut-off (avoidant).
ATTACHMENTS • Understanding your client’s attachment status is critical to breaking long held beliefs about close relationships or what Bowlby described as the internal working models of self and other”.
DANIEL SIEGEL :PROCESS OF EMOTION • THE BODY KNOWS WHAT ITS FEELING BEFORE THE MIND KNOWS • THE MIND PICKS UP THE MESSAGE RELAYING: “PAY ATTENTION, THIS IS IMPORTANT!” • THE MIND MAKES A DECISION—THIS IS GOOD OR THIS IS BAD(MOOD) • THIS PROCESS OF AFFECT(MOOD) CAN BE ELABORATED INTO CATEGORIES OF AFFECT:
CATEGORIES OF AFFECT • ANGER • FEAR • SURPRIZE • DISGUST • JOY • EXCITEMENT • SHAME • SEE NOTES ON SHAME(CLASS SET)
MOST COMUNICATIONS BETWEEN INFANT and PARENTS OR ADULTS IS PRIMARY AFFECT AS OPPOSES TO CATEGORICAL AFFECT. • MUCH IS SAID WITHOUT SAYING IT.
POSITIVE PARENTING • THOSE who grew up in healthy families where primary emotions/positive affect was shared and negative emotions/ primary affects soothed constructively are more sensitive to themselves and others.
LESS POSITIVE PARENTING • THOSE WITH LESS POSITIVE PARENTING ARE QUITE OUT OF TOUCH WITH OR UNABLE TO ARTICULATE THEIR PRIMARY AFFECTS AND THEIR CATEGORICAL EMOTIONS. • MUCH OF WHAT THEY ARE FEELING IS COMMUNICATED BEHAVIORALLY RATHER THAN WITH WORDS. • NOR ARE THEY SENSITIVE TO THE EMOTIONS OF OTHERS
IN THERAPY • Many clients have not learned the language of primary affect nor the language of categorical emotion • Many cannot discern primary affect communicated via facial expression, eye gaze, tone of voice, body motion, and timing of responses.
IN THERAPY THIS CAN BE: • TAUGHT • REFLECTED • PRACTICED
In therapy • Clients feel understood because their state of mind is being “felt” by another. • discussion & movie excerpt :IN THE BEDROOM
WHAT CONSTITUTES MOTIVATION FOR CHANGE • PRECONTEMPATION • CONTEMPLATION • PREPARATION • ACTION • MAINTENANCE • RELAPSE PREVENTION AND RESPONSE
AN INCORRECT MYSTIQUE • The idea that all individuals are in complete control of their behavior stems from the socio-political perspective that emphasizes • Power • Control • Self-will • Accountability • discussion
THE VAST MAJORITY OF BATTERERS NEED MORE THAN JUST THE MESSAGE: “ USE VIOLENCE…GO TO JAIL”.
Violence is a function of a complex interaction of biological, psychological, and social processes that require complex interventions. • Change takes time • New opportunities arise for deepening the work • Learning new coping skills • Refining and personalizing interventions • Securing safety
COMMON PSYCHOLOGICAL DIAGNOSES • Depression, anxiety or both • Psychoactive substance abuse and dependency • Posttraumatic stress disorder • Neurobiological disorders • Personality disorders
DUTTON’S BATTERY TYPOLOGY • OVER-CONTROLLED: deny rage while experiencing chronic frustration an resentment • UNDERCONTROLLED: act out frequently • INSTRUMENTAL: use violence “coldly” to obtain specific objectives • IMPULSIVE: • act out in response to a buiding inner psychological tension
Conditional model of violence prediction • Individual biological/psychological factors: • History of violence • Substance abuse • Need for medication • Psychiatric disorders
SOCIAL/ENVIRONMENTAL FACTORS • PEER support for violence(ie. Gangs) • Economic stressors • Occupational stressors
RATIOANAL FOR USING ATTACHMENT THEORY • Violence occurs in the context of attachment relationships • Anger and loss associated with maintenance of proximity • Very high rates amongst batterers with insecure attachment • High rates of childhood trauma among perpetrators and victims of violence(30-50% among victims).
PARENTS AND CHILDREN • Most parents, in their efforts to help their children, focus attention: • on decoding the child’s behavior yielding an expertise about the child • but also a blindness to their own contribution.
POWER • Violence is an ugly form of power in the face of which we all feel threatened. • 2 forms of violence • Violence to achieve a goal = coercive • Pleading violence in which the victimizer perceives himself/herself to be the victim
divorce • Children of divorce do scary things. • They have seen parents stop loving each other. • The possibility of abandonment terrifies them • Competition with new members ( step families) becomes very serious business, it’s survival of the fittest.
Rollo May’s levels of power These levels of power are seen as potentialities within everyone: The power to be-neither good nor evil, but NOT neutral. Power is energy. This energy must be lived out or it results impotently in death, neurosis, psychosis, or violence