Download

1 / 23
240 likes | 685 Views
EKG Monitoring . Types of EKG Monitoring. Critical Care 24 hours/day Immediate recognition of problems Cardiac stepdown 24 hours/day Immediate response 12 Lead EKG When needed Specific order or standing order. Continuos Monitoring. 3 to 5 electrodes are placed on chest

E N D
Types of EKG Monitoring • Critical Care • 24 hours/day • Immediate recognition of problems • Cardiac stepdown • 24 hours/day • Immediate response • 12 Lead EKG • When needed • Specific order or standing order
Continuos Monitoring • 3 to 5 electrodes are placed on chest • Must change pads prevent irritation according to policy • Monitor tech watches for changes • Can determine rate, rhythm and changes
12 Lead EKG • Used to determine both new and old heart problems • Electricity is conducted differently over injured heart muscle • Determines rate, rhythm and changes from previous EKG • Looks at heart in 12 directions • Usually done by trained personnel • Current flows from a negative to a positive lead • The lead placement determines the direction of the deflection of the QRS complex
Interpretation of an EKG • Graph paper divided into small and large squares • Each small square represents 0.04 seconds on the horizontal axis and I mm on the vertical axis • Each large square contains 5 small squares and represents 0.20 seconds and 5 mm • The electrical activity is recognized by upward and downward deflections of the wave forms • The baseline is called the isoelectric line
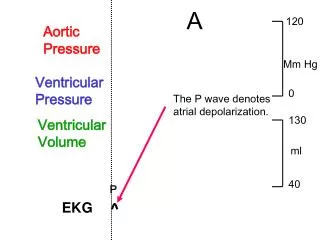
Interpretation of an EKG, cont. • P Wave- represents atrial depolarization and is the 1st deflection and indicates the results of the SA node firing • PR interval – represents time required for atrial repolarization and the time it takes for the impulse to travel from the atria to the ventricles (normal is 0-.12 to 0.20 seconds) • QRS complex – represents ventricular depolarization (normal is 0.06 to 0.10 seconds) • T Wave– represents ventricular repolarization
Interpretation of an EKG, cont • EKG is evaluated for • Rate – done on EKG by using the 6 second strip from R wave to R wave (normal is 60-100) • Regularity – measure for consistency • P waves – look for a P wave before each QRS complex • PR interval – must fall in the normal range • QRS complexes – must be normal or may be problem in the conduction system • T waves – should be rounded, upright and same shape and size (not inverted )
Systematic Review of EKG Strip • Determine rate and regularity • Is there a P wave before each QRS complex • Are P waves rounded and upright • Measure the QRS and do they look alike • Look at the T wave. Is it upright or inverted
Common Dysrhythmias • Sinus dysrhythmias • Sinus tachycardia – greater than 100 • Sinus bradycardia – less than 60 • Sinus arrest • Atrial dysrhythmias • PAC • SVT • Atrial fibrillation • Atrial flutter
Common Dysrhythmias, cont. • Atrioventricular blocks • 1st degree, 2nd degree, and 3rd degree AV block • Ventricular dysrhythmias • V-tache • V-fib • PVC’s • Idioventricular • Ventricular asystole
Treatment • Based on severity of the problem • Lethal dysrhythmias are treated immediately • Asystole – Atropine, Epinephrine • V-tache – lidocaine, Pronestyl, mag sulfate, amiodarone • V-fib – defibrillation with drugs • Some may cause severe symptoms while others do not
Quinidine Pronestyl Lidocaine Mexitil Tonocard Tambocor Rythmol Adenocard Magnesium sulfate Inderal Brevibloc Betapace Cordarone Covert Verapamil Cardizem Lanoxin Atropine Drug Treatment of Dysrhythmias
Pacemakers • Used to restore regular rhythm and improve cardiac output • Types • Temporary • Permanent • Transcutaneous • Transvenous • Implantable
Modes of Delivery • Single chamber • Duel chamber • Fixed rate • Demand rate • AV sequential
Care of Pacemaker • Vitals on return from OR • Check insertion site and provide care as needed • Monitor for: • rhythm • pacemaker spike • PVC’s or other abnormal beats • Usually on bedrest for 24 hours , off the side of insertion • Gradually increase activities • Patient must carry ID card • Instruct patient to take pulse daily • Notify physician both in hospital and after home of: • Dyspnea • Syncope • Dizziness • Weakness • Fatigue • Chest pain
Implantable Cardioverter/Defibrillator • Used to treat life threatening rhythm problems • Senses heart rate and wave form and delivers a shock to return heart function to a regular rhythm • Recognizes V-tach and V-Fib • If rhythm does not return to NSR, can continue • Newer models can also recognize tachyarrhythmias and bradyarrhythmias • Implanted in the sub-q tissue over the pectoralis muscle • Causes some anxiety to patient when shock delivered • Family and patient need education and support • Wears ID bracelet • Should avoid heavy magnetic fields (MRI, metal detectors)