Download

1 / 76
800 likes | 1.41k Views
HEART. BY DR ABIODUN MARK AKANMODE. CONTENT. Normal heart physiology and anatomy. Heart failure. Congenital heart diseases. Ischemic heart diseases. Hypertensive heart diseases. Valvular heart diseases. Endocarditis . Cardiomyopaties . Myocarditis . Miscellaneous. Normal heart.

E N D
HEART BY DR ABIODUN MARK AKANMODE.
CONTENT. • Normal heart physiology and anatomy. • Heart failure. • Congenital heart diseases. • Ischemic heart diseases. • Hypertensive heart diseases. • Valvular heart diseases. • Endocarditis. • Cardiomyopaties. • Myocarditis. • Miscellaneous.
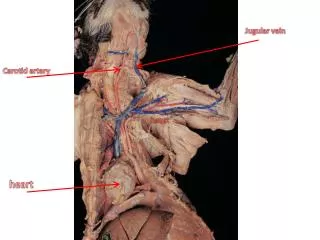
Normal heart • This is the external appearance of a normal heart. • The epicardial surface is smooth and glistening. The amount of epicardial fat is usual. • The left anterior descending coronary artery extends down from the aortic root to the apex.
Myocardial(NORMAL) • This is the normal appearance of myocardial fibers in longitudinal section. • Note the central nuclei and the syncytial arrangement of the fibers, some of which have pale pink intercalated disks.
Heart failure (HF) • Congestive heart failure (CHF) or congestive cardiac failure (CCF), occurs when the heart is unable to provide sufficient pump action to maintain blood flow to meet the needs of the body. • The condition is diagnosed by patient physical examination and confirmed with echocardiography. • In a chronic patient already in a stable situation, treatment commonly consists of lifestyle measures such as smoking cessation, light exercise, dietary changes, and medications. • Generally CCF can be divided into RHF and LHF.
RSF. • RSF is mostly caused by LSF. • Isolated RSF is caused by intrinsic conditions that increase the pressure within the lungs also tricuspid or pulmonary valvular diseases can lead to increase pressure on lungs ultimately causing pulmonary HTN. • This is referred to as corpulmonale.(i.e. RSF due to pulmonary hypertension)
LHF. • The major causes of LHF are ischemic heart diseases, hypertension, aortic and mitral valve diseases etc. • LHF is manifested classically by pulmonary edema & congestion. • Reduced renal perfusion due to decreased cardiac output. • Reduced CNS perfusion causing hypoxic encephalopathy which could range from mare irritability to severe coma.
CHD. • CHD refers to cardiac or great vessel abnormalities that are present at birth. • Most of the CHD are attributed to faulty embryogenesis between the 3rd and 8th week of gestation when major organs like the heart develops. • CHD are of 2 types.-Shunts.-obstructions.
CHD-SHUNTS. • Shuts can be of 2 types. • Left to right shunts(late cyanosis or blue kids)e.g.: ASD(atrialseptal defects) VSD(ventricular septal defect) PDA(patent ductusarteriosus) • Right to left shunts(early cyanosis or blue babies)e.g.: TOF(tetralogy of fallot)TG(transposition of great vessels) PTA.(persistent truncusarteriosus) TAVPR.(total anomalous venous pulmonary return) TA.(tricuspid atresia)
CHD-OBSTRUCTION. • Obstructive congenital diseases include: • Aortic coarctation which can either be preductal or postductal. • Valvularstenosis and atresias. • Obstructive congenital diseases are generally not associated with cyanosis.
IHD(ISCHEMIC HEART DISEASES) • This refers to a group of closely related heart diseases resulting from ischemia. • Ischemia here is not just oxygen insufficiency but nutrients and metabolites also. • Basically there is a mismatch between cardiac demands and vascular supply. • The 4 basic IHD are: Myocardial infarction. Angina pectoris. Chronic ischemic HD Sudden cardiac death.
MYOCARDIAL INFARCTION. • MI the most important form of IHD generally occurs when the duration and severity of ischemia is sufficient to cause the death of cardiac muscle cells. • MI can be of 2 types.-transmural MI: involves all layers of the heart.-Subendocardialinfact: does not involve all layers.
Contraction band necrosis in MI. • The earliest change histologically seen with acute myocardial infarction in the first day is contraction band necrosis. • The myocardial fibers are beginning to lose cross striations and the nuclei are not clearly visible in most of the cells seen here. • Note the many irregular darker pink wavy contraction bands extending across the fibers.
Complications of MI. • Fatal arrytmias. • CHF. • Cardiogenic shock. • Ventricular free wall rupture causing pericardial tamponade. • Fibrinouspericarditis. • Dressler’s syndrome.
Ventricular wall Rupture. • One complication of a transmural myocardial infarction is rupture of the myocardium. • This is most likely to occur in the first week between 3 to 5 days following the initial event, when the myocardium is the softest. • Note the dark red blood clot forming the hemopericardium. • The hemopericardium can lead to tamponade.
Coronary artery bypass grafting • This patient underwent coronary artery bypass grafting with autogenous vein (saphenous vein) grafts. • The largest of these runs down the center of the heart to anastomose with the left anterior descending artery distally. • The internal mammary artery can also be harvested for CABG. • The internal mammary artery has a better 10 yr prognosis as compared to the saphenous vein.
HHD. • Hypertensive heart diseases mostly affects the left ventricle. • In the setting of chronic hypertension the workload on the ventricles is increases and since he heart muscles cannot divide or replicate(permanent cells) they undergo hypertrophy so as to maintain cardiac function. • Here the ventricular wall is thickened (>2cm) and the heart weight is greater than 550gm.
VALVULAR HEART DISEASES. • VHD in adults is typically caused by degeneration(e.gcalcific aortic stenosis, mitral anular calcification, mitral valve prolapse),immunologic inflammatory processes (e.g rheumatic heart diseases etc) or infections. • Degenerative calcific aortic valve stenosis. • Mitral valve prolapse.
Endocarditis. • Endocarditis is an inflammation of the inner layer of the heart, the endocardium. It usually involves the heart valves (native or prosthetic valves). • Other structures that may be involved include the interventricular septum, the chordaetendineae, the mural endocardium, or even the surfaces of intracardiac devices. • Endocarditis is characterized by a prototypic lesion, the vegetation, which is a mass of platelets, fibrin, microcolonies of microorganisms, and scant inflammatory cells
Types of Endocarditis. • Infective endocarditis: here microbes colonize the heart valves and forms friable vegetations. The 2 types of infective endocarditis are acute and subacute.Diagnosis is via the Duke’s criteria. • Non bacterial thrombotic endocarditis aka maranticendocarditis: this variant characteristically occurs in the settings of cancers e.g. adenocarcinomas • Libman sacks endocarditis: occurs with systemic diseases like SLE and antiphospholipid syndrome.
Maranticendocarditis/NBTE. • The small pink vegetation on the rightmost cusp margin represents the typical finding with non-bacterial thrombotic endocarditis (or so-called "maranticendocarditis"). • This is non-infective. It tends to occur in persons with a hypercoagulable state and in some malignancies.
Verrucous vegetations in LBE. • The small verrucous vegetations seen along the closure line of this mitral valve are associated with SLE LIBMAN SACKS ENDOCARDITIS. • These warty vegetations average only a few millimeters and form along the line of valve closure over areas of endocardial inflammation. Such verrucae are too small to cause serious cardiac problems.
Dilated cardiomyopathy • Here is a large, dilated left ventricle typical of a dilated, or congestive, cardiomyopathy. Many of these have no known etiology (so-called "idiopathic dilated cardiomyopathy") while others may be associated with chronic alcoholism. The heart is very enlarged and flabby. • Microscopically, the heart in cardiomyopathy demonstrates hypertrophy of myocardial fibers (which also have prominent dark nuclei) along with interstitial fibrosis.