Download
1 / 1
10 likes | 126 Views
Dizziness Among Elderly Patients Admitted in a Tertiary Hospital Fritz Rinaldi DA. Bernardo, MD and Artemio A. Roxas Jr., MD, FPNA Section of Adult Neurology, The Medical City. ABSTRACT

E N D
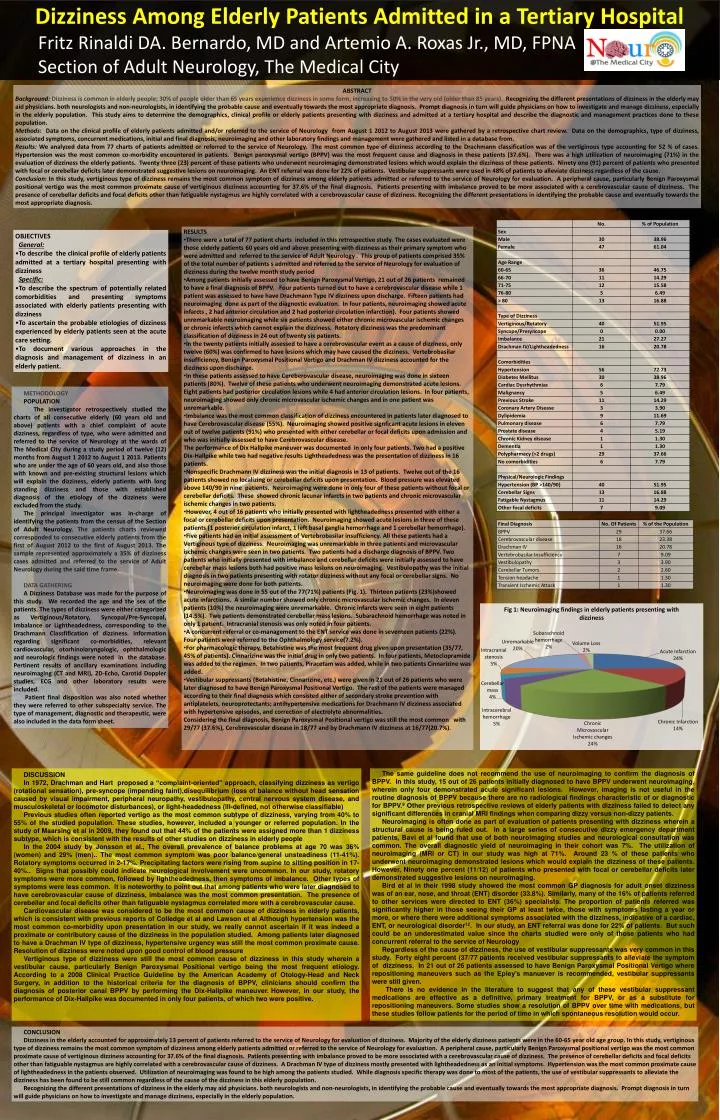
Dizziness Among Elderly Patients Admitted in a Tertiary Hospital Fritz Rinaldi DA. Bernardo, MD and Artemio A. Roxas Jr., MD, FPNA Section of Adult Neurology, The Medical City ABSTRACT Background:Dizziness is common in elderly people; 30% of people older than 65 years experience dizziness in some form, increasing to 50% in the very old (older than 85 years). Recognizing the different presentations of dizziness in the elderly may aid physicians. both neurologists and non-neurologists, in identifying the probable cause and eventually towards the most appropriate diagnosis. Prompt diagnosis in turn will guide physicians on how to investigate and manage dizziness, especially in the elderly population. This study aims to determine the demographics, clinical profile or elderly patients presenting with dizziness and admitted at a tertiary hospital and describe the diagnostic and management practices done to these population. Methods: Data on the clinical profile of elderly patients admitted and/or referred to the service of Neurology from August 1 2012 to August 2013 were gathered by a retrospective chart review. Data on the demographics, type of dizziness, associated symptoms, concurrent medications, initial and final diagnosis, neuroimaging and other laboratory findings and management were gathered and listed in a database from. Results: We analyzed data from 77 charts of patients admitted or referred to the service of Neurology. The most common type of dizziness according to the Drachmann classification was of the vertiginous type accounting for 52 % of cases. Hypertension was the most common co-morbidity encountered in patients. Benign paroxysmal vertigo (BPPV) was the most frequent cause and diagnosis in these patients (37.6%). There was a high utilization of neuroimaging (71%) in the evaluation of dizziness the elderly patients. Twenty three (23) percent of these patients who underwent neuroimaging demonstrated lesions which would explain the dizziness of these patients. Ninety one (91) percent of patients who presented with focal or cerebellar deficits later demonstrated suggestive lesions on neuroimaging. An ENT referral was done for 22% of patients. Vestibular suppressants were used in 48% of patients to alleviate dizziness regardless of the cause. Conclusion: In this study, vertiginous type of dizziness remains the most common symptom of dizziness among elderly patients admitted or referred to the service of Neurology for evaluation. A peripheral cause, particularly Benign Paroxysmal positional vertigo was the most common proximate cause of vertiginous dizziness accounting for 37.6% of the final diagnosis. Patients presenting with imbalance proved to be more associated with a cerebrovascular cause of dizziness. The presence of cerebellar deficits and focal deficits other than fatiguablenystagmus are highly correlated with a cerebrovascular cause of dizziness. Recognizing the different presentations in identifying the probable cause and eventually towards the most appropriate diagnosis. • RESULTS • There were a total of 77 patient charts included in this retrospective study. The cases evaluated were those elderly patients 60 years old and above presenting with dizziness as their primary symptom who were admitted and referred to the service of Adult Neurology . This group of patients comprised 35% of the total number of patients s admitted and referred to the service of Neurology for evaluation of dizziness during the twelve month study period • Among patients initially assessed to have Benign Paroxysmal Vertigo, 21 out of 26 patients remained to have a final diagnosis of BPPV. Four patients turned out to have a cerebrovascular disease while 1 patient was assessed to have have Drachmann Type IV dizziness upon discharge. Fifteen patients had neuroimaging done as part of the diagnostic evaluation. In four patients, neuroimaging showed acute infarcts , 2 had anterior circulation and 2 had posterior circulation infarction). Four patients showed unremarkable neuroimaging while six patients showed either chronic microvascular ischemic changes or chronic infarcts which cannot explain the dizziness. Rotatory dizziness was the predominant classification of dizziness in 24 out of twenty six patients. • In the twenty patients initially assessed to have a cerebrovascular event as a cause of dizziness, only twelve (60%) was confirmed to have lesions which may have caused the dizziness. Vertebrobasilar insufficiency, Benign Paroxysmal Positional Vertigo and Drachman IV dizziness accounted for the dizziness upon discharge. • In these patients assessed to have Cereberovascular disease, neuroimaging was done in sixteen patients (80%). Twelve of these patients who underwent neuroimaging demonstrated acute lesions. Eight patients had posterior circulation lesions while 4 had anterior circulation lesions. In four patients, neuroimaging showed only chronic microvascular ischemic changes and in one patient was unremarkable. • Imbalance was the most common classification of dizziness encountered in patients later diagnosed to have Cerebrovascular disease (55%). Neuroimaging showed positive signficant acute lesions in eleven out of twelve patients (91%) who presented with either cerebellar or focal deficits upon admission and who was initially assessed to have Cerebrovascular disease. • The performance of Dix Hallpike maneuver was documented in only four patients. Two had a positive Dix-Hallpike while two had negative results Lightheadedness was the presentation of dizziness in 16 patients. • Nonspecific Drachmann IV dizziness was the initial diagnosis in 13 of patients. Twelve out of the 16 patients showed no localizing or cerebellar deficits upon presentation. Blood pressure was elevated above 140/90 in nine patients. Neuroimaging were done in only four of these patients without focal or cerebellar deficits. These showed chronic lacunar infarcts in two patients and chronic microvascular ischemic changes in two patients. • However, 4 out of 16 patients who initially presented with lightheadedness presented with either a focal or cerebellar deficits upon presentation. Neuroimaging showed acute lesions in three of these patients (1 posterior circulation infarct, 1 left basal ganglia hemorrhage and 1 cerebellar hemorrhage). • Five patients had an initial assessment of Vertebrobasilar insufficiency. All these patients had a Vertiginous type of dizziness. Neuroimaging was unremarkable in three patients and microvascular ischemic changes were seen in two patients. Two patients had a discharge diagnosis of BPPV. Two patients who initially presented with imbalance and cerebellar deficits were initially assessed to have cerebellar mass lesions both had positive mass lesions on neuroimaging. Vestibulopathy was the initial diagnosis in two patients presenting with rotator dizziness without any focal or cerebellar signs. No neuroimaging were done for both patients. • Neuroimaging was done in 55 out of the 77(71%) patients (Fig. 1). Thirteen patients (23%)showed acute infarctions. A similar number showed only chronic microvascular ischemic changes. In eleven patients (10%) the neuroimaging were unremarkable. Chronic infarcts were seen in eight patients (14.5%). Two patients demonstrated cerebellar mass lesions. Subarachnoid hemorrhage was noted in only 1 patient. Intracranial stenosis was only noted in four patients. • A concurrent referral or co-management to the ENT service was done in seventeen patients (22%). Four patients were referred to the Ophthalmology service(7.2%). • For pharmacologic therapy, Betahistine was the most frequent drug given upon presentation (35/77, 45% of patients). Cinnarizine was the initial drug in only two patients. In four patients, Metoclopramide was added to the regimen. In two patients, Piracetam was added, while in two patients Cinnarizine was added. • Vestibular suppressants (Betahistine, Cinnarizine, etc.) were given in 21 out of 26 patients who were later diagnosed to have Benign Paroxysmal Positional Vertigo. The rest of the patients were managed according to their final diagnosis which consisted either of secondary stroke prevention with antiplatelets, neuroprotectants; antihypertensive medications for Drachmann IV dizziness associated with hypertensive episodes, and correction of electrolyte abnormalities. • Considering the final diagnosis, Benign Paroxysmal Positional vertigo was still the most common with 29/77 (37.6%), Cerebrovascular disease in 18/77 and by Drachmann IV dizziness at 16/77(20.7%). OBJECTIVES General: • To describe the clinical profile of elderly patients admitted at a tertiary hospital presenting with dizziness Specific: • To describe the spectrum of potentially related comorbidities and presenting symptoms associated with elderly patients presenting with dizziness • To ascertain the probable etiologies of dizziness experienced by elderly patients seen at the acute care setting. • To document various approaches in the diagnosis and management of dizziness in an elderly patient. METHODOLOGY POPULATION The investigator retrospectively studied the charts of all consecutive elderly (60 years old and above) patients with a chief complaint of acute dizziness, regardless of type, who were admitted and referred to the service of Neurology at the wards of The Medical City during a study period of twelve (12) months from August 1 2012 to August 1 2013. Patients who are under the age of 60 years old, and also those with known and pre-existing structural lesions which will explain the dizziness, elderly patients with long standing dizziness and those with established diagnosis of the etiology of the dizziness were excluded from the study. The principal investigator was in-charge of identifying the patients from the census of the Section of Adult Neurology. The patients charts reviewed corresponded to consecutive elderly patients from the first of August 2012 to the first of August 2013. The sample represented approximately a 35% of dizziness cases admitted and referred to the service of Adult Neurology during the said time frame. DATA GATHERING A Dizziness Database was made for the purpose of this study. We recorded the age and the sex of the patients. The types of dizziness were either categorized as Vertiginous/Rotatory, Syncopal/Pre-Syncopal, Imbalance or Lightheadedness, corresponding to the Drachmann Classfification of dizziness. Information regarding significant co-morbidities, relevant cardiovascular, otorhinolaryngologic, ophthalmologic and neurologic findings were noted in the database. Pertinent results of ancillary examinations including neuroimaging (CT and MRI), 2D-Echo, Carotid Doppler studies, ECG and other laboratory results were included. Patient final disposition was also noted whether they were referred to other subspecialty service. The type of management, diagnostic and therapeutic, were also included in the data form sheet. DISCUSSION In 1972, Drachman and Hart proposed a “complaint-oriented” approach, classifying dizziness as vertigo (rotational sensation), pre-syncope (impending faint),disequilibrium (loss of balance without head sensation caused by visual impairment, peripheral neuropathy, vestibulopathy, central nervous system disease, and musculoskeletal or locomotor disturbances), or light-headedness (ill-defined, not otherwise classifiable) • Previous studies often reported vertigo as the most common subtype of dizziness, varying from 40% to 55% of the studied population. These studies, however, included a younger or referred population. In the study of Maarsing et al in 2009, they found out that 44% of the patients were assigned more than 1 dizziness subtype, which is consistent with the results of other studies on dizziness in elderly people • In the 2004 study by Jonsson et al.,The overall prevalence of balance problems at age 70 was 36% (women) and 29% (men).. The most common symptom was poor balance/general unsteadiness (11-41%). Rotatory symptoms occurred in 2-17%. Precipitating factors were rising from supine to sitting position in 17-40%.. Signs that possibly could indicate neurological involvement were uncommon. In our study, rotatory symptoms were more common, followed by lightheadedness, then symptoms of imbalance. Other types of symptoms were less common. It is noteworthy to point out that among patients who were later diagnosed to have cerebrovascular cause of dizziness, imbalance was the most common presentation. The presence of cerebellar and focal deficits other than fatiguablenystagmus correlated more with a cerebrovascular cause. • Cardiovascular disease was considered to be the most common cause of dizziness in elderly patients, which is consistent with previous reports of Colledge et al and Lawson et alAlthough hypertension was the most common co-morbidity upon presentation in our study, we really cannot ascertain if it was indeed a proximate or contributory cause of the dizziness in the population studied. Among patients later diagnosed to have a Drachman IV type of dizziness, hypertensive urgency was still the most common proximate cause. Resolution of dizziness were noted upon good control of blood pressure • Vertiginous type of dizziness were still the most common cause of dizziness in this study wherein a vestibular cause, particularly Benign Paroxysmal Positional vertigo being the most frequent etiology. According to a 2008 Clinical Practice Guideline by the American Academy of Otology-Head and Neck Surgery, in addition to the historical criteria for the diagnosis of BPPV, clinicians should confirm the diagnosis of posterior canal BPPV by performing the Dix-Hallpikemaneuver.However, in our study, the performance of Dix-Hallpike was documented in only four patients, of which two were positive. • The same guideline does not recommend the use of neuroimaging to confirm the diagnosis of BPPV. In this study, 15 out of 26 patients initially diagnosed to have BPPV underwent neuroimaging, wherein only four demonstrated acute significant lesions. However, imaging is not useful in the routine diagnosis of BPPV because there are no radiological findings characteristic of or diagnostic for BPPV.9 Other previous retrospective reviews of elderly patients with dizziness failed to detect any significant differences in cranial MRI findings when comparing dizzy versus non-dizzy patients. • Neuroimaging is often done as part of evaluation of patients presenting with dizziness wherein a structural cause is being ruled out. In a large series of consecutive dizzy emergency department patients, Bavi et al found that use of both neuroimaging studies and neurological consultation was common. The overall diagnostic yield of neuroimaging in their cohort was 7%. The utilization of neuroimaging (MRI or CT) in our study was high at 71%. Around 23 % of these patients who underwent neuroimaging demonstrated lesions which would explain the dizziness of these patients. However, Ninety one percent (11/12) of patients who presented with focal or cerebellar deficits later demonstrated suggestive lesions on neuroimaging. • Bird et al in their 1998 study showed the most common GP diagnosis for adult onset dizziness was of an ear, nose, and throat (ENT) disorder (33.8%). Similarly, many of the 16% of patients referred to other services were directed to ENT (36%) specialists. The proportion of patients referred was significantly higher in those seeing their GP at least twice, those with symptoms lasting a year or more, or where there were additional symptoms associated with the dizziness, indicative of a cardiac, ENT, or neurological disorder12. In our study, an ENT referral was done for 22% of patients. But such could be an underestimated value since the charts studied were only of those patients who had concurrent referral to the service of Neurology • Regardless of the cause of dizziness, the use of vestibular suppressants was very common in this study. Forty eight percent (37/77 patients received vestibular suppressants to alleviate the symptom of dizziness. In 21 out of 26 patients assessed to have Benign Paroxysmal Positional Vertigo where repositioning maneuvers such as the Epley’smanuever is recommended, vestibular suppressants were still given. • There is no evidence in the literature to suggest that any of these vestibular suppressant medications are effective as a definitive, primary treatment for BPPV, or as a substitute for repositioning maneuvers. Some studies show a resolution of BPPV over time with medications, but these studies follow patients for the period of time in which spontaneous resolution would occur. CONCLUSION Dizziness in the elderly accounted for approximately 13 percent of patients referred to the service of Neurology for evaluation of dizziness. Majority of the elderly dizziness patients were in the 60-65 year old age group. In this study, vertiginous type of dizziness remains the most common symptom of dizziness among elderly patients admitted or referred to the service of Neurology for evaluation. A peripheral cause, particularly Benign Paroxysmal positional vertigo was the most common proximate cause of vertiginous dizziness accounting for 37.6% of the final diagnosis. Patients presenting with imbalance proved to be more associated with a cerebrovascular cause of dizziness. The presence of cerebellar deficits and focal deficits other than fatiguablenystagmus are highly correlated with a cerebrovascular cause of dizziness. A Drachman IV type of dizziness mostly presented with lightheadedness as an initial symptoms. Hypertension was the most common proximate cause of lightheadedness in the patients observed. Utilization of neuroimaging was found to be high among the patients studied. While diagnosis specific therapy was done to most of the patients, the use of vestibular suppressants to alleviate the dizziness has been found to be still common regardless of the cause of the dizziness in this elderly population. Recognizing the different presentations of dizziness in the elderly may aid physicians. both neurologists and non-neurologists, in identifying the probable cause and eventually towards the most appropriate diagnosis. Prompt diagnosis in turn will guide physicians on how to investigate and manage dizziness, especially in the elderly population.