Download
1 / 60
880 likes | 2.19k Views
Cardiac reflexes and implications in anaesthetic practice. Dr. Anuradha Patel. University College of Medical Sciences & GTB Hospital, Delhi. Cardiac Reflex. Fast acting reflex loops between the heart and CNS Regulates cardiac function Maintains physiologic homeostasis

E N D
Cardiac reflexes and implications in anaesthetic practice Dr. Anuradha Patel University College of Medical Sciences & GTB Hospital, Delhi
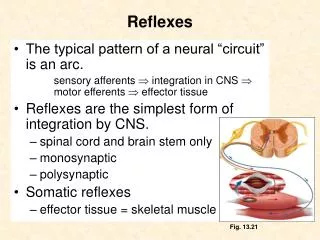
Cardiac Reflex • Fast acting reflex loops between the heart and CNS • Regulates cardiac function • Maintains physiologic homeostasis • Cardiac receptors are linked to CNS by myelinated / unmyelinated afferents of vagus nerve • Cardiac receptors are present in • Atria • Ventricles • Pericardium • Coronary arteries
Cardiac receptor Myelinated / unmyelinated afferent of vagus nerve Central processing of sympathetic and parasympathetic nerve input in the CNS Efferent fibres Heart or systemic circulation Particular reaction
Afferent fibres of cardiac receptors (in vagus nerve) Myelinated fibres (25%) Unmyelinated fibres (75%) Present in walls of atria and atriocaval junction Present in walls of all cardiac chambers
Cardiac innervation • Sympathetic nerve – noradrenergic fiber; Parasympathetic nerve- cholinergic fiber • Noradrenergic sympathetic nerve • to the heart increase the cardiac rate (chronotropic effect) • the force of cardiac contraction (inotropic effect). • Cholinergic vagal cardiac fibers decrease the heart rate.
Cardiovascular Reflexes • Baroreceptor reflex (carotid sinus reflex) (pressure receptor reflex) • Chemoreceptor reflex • Bainbridge atrial reflex (volume reflex) (atrial stretch reflex) • Bezold-Jarisch reflex (cardiopulmonary reflex) • Oculocardiac reflex (trigeminovagal reflex) • Cushing’s reflex • Valsalva maneuver
Baroreceptor Reflex (carotid sinus reflex) (pressor receptor reflex) • Reflex initiated by stretch receptors, called baroreceptors or pressor receptors • Baroreceptors are present in • Carotid sinus • Aortic arch • Walls of right atrium at the entrance of SVC and IVC • Walls of left atria at the entrance of pulmonary vein • These receptors in low pressure part of the circulation are called as cardiopulmonary receptors • They are stimulated by distension of the structure in which they are located • pressure in these structures are associated with discharge rate
Carotid sinus At the bifurcation of the common carotid arteries the root of internal carotid artery shows a little bulge has stretch receptors in the adventitia are sensitive to arterial pressure fluctuations Afferent nerves from these stretch receptors travel in the carotid sinus nerve which is a branch of the glossopharyngeal nerve (IXth cranial nerve)
Aortic Arch • baroreceptors are also present in the adventitia of the arch of aorta • have functional characteristics similar to the carotid sinus receptors. • their afferent nerve fibers travel in the aortic nerve, • branch of the vagus nerve. (Xth cranial nerve)
Basic pathways involved in the medullary control of heart rate by the vagus nerves
Buffer nerves activity • The carotid sinus nerves and vagal fibers from the aortic arch are commonly called the buffer nerves • At normal blood pressure levels, the fibers of the buffer nerve discharge at a low rate. • When the pressure in the sinus and aortic arch rises, the discharge rate increases; • when the pressure falls, the rate declines.
Discharges (vertical lines) in a single afferent nerve fiber from the carotid sinus at various levels of mean MAP, plotted against changes in aortic pressure with time
Fall in systemic blood pressure produced by raising the pressure in the isolated carotid sinus of a normal monkey to various values
Activation of the baroreceptors at different levels of arterial pressure. I, change in carotid sinus nerve impulses per second; P, change in arterial blood pressure in mm Hg.
Baroreceptors respond extremely rapidly to changes in BP (within fraction of seconds) • Response much more to rapidly changing BP than to stationary pressure • Maintains BP through a negative feedback loop
Importance of the baroreceptor reflex • To keep the arterial pressure relatively constant • Short term regulation of blood pressure in the range of 70 mmHg to 150 mmHg, maintain the mean blood pressure at about 100 mmHg • Pressure buffer system – reduce the blood fluctuation during the daily events, such as changing of the posture, respiration and excitement
Baroreceptor Resetting • Baroreceptor will adapt to the long term change of blood pressure. • That is, if the blood pressure is elevated for a longer time, as in chronic HTN, the set point will transfer to the elevated mean blood pressure • So there is decrease baroreceptor response in pts with chronic HTN • This makes the baroreceptor system unimportant for long-term regulation of arterial pressure
CCBs, ACE-inhibitors, PDE inhibitors - cardiovascular response of increasing BP through this reflex Baroreceptors are compromised by diabetic neuropathy Volatile anaesthetics (particularly halothane) inhibit HR component of the reflex These reflexes are well preserved with moderate doses of fentanyl but high doses depresses this reflex
Chemoreceptor Reflexes Mediated by • Peripheral chemoreceptors • Carotid bodies • Aortic bodies • Central chemoreceptors • Medulla (associated with cardiovascular control “centers”) • Sinus nerve of Hering (branch of 9th cranial nerve) and vagus nerve
Peripheral Chemoreceptors • Present in carotid & aortic bodies • 2 mm in size • Supplied with abundant blood flow through a small nutrient artery (senses changes in BP) • Rich sensory innveration • Rate of response is fast
Chemoreceptor areas in carotid and aortic bodies CAROTID BODY AORTIC BODY
Respiratory control by peripheral chemoreceptors in the carotid and aortic bodies
Carotid bodies • 2 in number • 2 mg weight • Highest blood flow – 2000 ml/100 g/min • Present at bifurcation of each common carotid artery • Innervated by sinus nerve (branch of 9th nerve) Aortic bodies • 1-3 in numbers • Adjacent to aorta • Near the aortic arch • Near root of subclavian artery • Innervated by 10th nerve
Central chemoreceptoprs – medulla (slow response) Cardiac control centres in medulla oblongeta Cardioaccelerator stimulatory centre (VMC) Cardioaccelerator inhibitory centre (CIC) Sympathetic stimulation Parasympathetic stimulation
Cardiovascular centers of the brainstem • Medulla oblongata is essential to Cardiovascular centers
Central & peripheral chemoreceptors respond to changes in chemical composition of blood or surrounding fluid • Central chemoreceptors respond only to acidosis • Peripheral chemoreceptors are sensitive to changes in arterial O2 and CO2 tension and to pH • Increasingly important when mean arterial pressure falls below 60 mmHg (i.e. when arterial baroreceptor firing rate is at minimum)
PaO2 < 50 mmHg / acidosis / PaCO2 Stimulate chemoreceptor in carotid & aortic bodies Sinus nerve of Hering & vagus nerve Medullary vasomotor centres Stimulate respiratory centres Directly stimulates sympathetic system Indirectly catecholamine secretion from the adrenal medulla pulm ventilation BP BP
Bainbridge Atrial Reflex(atrial stretch reflex, volume reflex) vagal tone right sided filling pressure Stretching of atria Stimulates stretch receptors present in right atrial wall & cavoatrial junction Vagal myelinated afferent fibres Directly stimulates SA node Cardiovascular center of medulla HR Efferents of vagus nerve Inhibit parasympathetic activity HR
Bainbridge Atrial Reflex Spinal or epidural anaesthesia Venous pooling in periphery Decreased stimulation of cardiac stretch receptor Decreased activity of cardiac sympathetic nerve Vagal predominance Decease heart rate
Reflex depends upon the preexisting heart rate • With slow heart rate, it causes progressive tachycardia • With pre-existing tachycardia, there is no effect • It helps prevent collection of blood in veins, atria and pulmonary circulation • It inhibits ADH release and promote secretion of ANP • Denervation of vagi to heart eliminate this reflex • The Bainbridge and baroreceptor reflex acts antagonistically to control heart rate • When blood volume is increased, the Bainbridge reflex is dominant, when it is decreased, baroreceptor reflex is dominant
Bezold-Jarisch reflex(cardiopulmonary reflex) Reflex triggered by • Intracoronary injection of veratrum alkaloids, serotonin, nicotine, capsaicin, phenyldiguamide • Coronary ischemia (MI) • Bradykinin, PGI2, Arachidonic acid • Ventricular distension • Coronary angioplasty • Thrombolysis • Revascularization • Syncope
Bezold-Jarisch reflex(cardiopulmonary reflex) Triggering factors Stimulates cardiopulmonary chemoreceptors and mechanoreceptors of LV wall Unmyelinated vagal afferent type C fibres Inhibit medullary vasomotor centre parasympathetic tone Triad of – bradycardia, hypotension, peripheral vasodilatation
Bezold-Jarisch reflex • Responsible for hypotension during regional anaesthesia
MI / Coronary reperfusion Molecules generated during ischemia and reperfusion such as free radicals and PG Stimulate cardiac inhibitory receptors(present in inferior & posterior walls of heart) Hypotension Bradycardia and renal vasodilatation Sudden cardiac death Decreases myocardial oxygen demand and augments renal perfusion (protective reflex)
Cardio-protective reflex, regulates BP in conjunction with baroreceptor reflex • Less pronounced in patients with cardiac hypertrophy & AF • Veratrum alkaloid can be used as an antihypertensive agent • Reflex dangerous in acute MI, coronary angiography, aortic stenosis and vaso-vagal syncope
Prevention • Prophylactic blockers Treatment • blockers & vagolytics (e.g. disopyramide) • Atropine for bradycardia
Oculocardiac Reflex(Trigemino-vagal Reflex, Aschner Phenomenon, Aschner Reflex, Aschner Dagini Reflex) Reflex triggered by Pressure on globe Traction on the extraocular muscle (esp. medial rectus muscle) as in strabismus surgery Ocular trauma Severe pain Orbital compression due to hematoma or edema Procedures under topical anaesthesia Orbital injections Hypercapnia or hypoxemia Fentanyl, sufentanil and remifentanil
Pressure on the globe of the eye or traction on the extraocular muscles Stimulates stretch receptors of extraocular muscle Afferents of short and long ciliary nerves Ciliary ganglion Ophthalmic division of trigeminal nerve Gasserian ganglion Sensory nucleus of trigeminal in the floor of 4th ventricle Efferents of vagus nerves (vagal cardiac depressor nerve) Parasympathetic stimulation Bradycardia / hypotension / asystole / AV block / ventricular ectopy
Treatment Immediate Cessation of manipulation IV atropine: 0.005 – 0.4 mg/kg or 7 µg/kg increments Lignocaine infiltration – near extrinsic muscles in case of recurrence IV epinephrine 6-12 mg for hypotension Prevention Indicated in patients with h/o conduction block, vaso-vagal responses or -blocker therapy Premedication with anti-cholinergics (atropine or glycopyrrolate) (block efferent pathway) Retrobulbar block with 1-3 ml of 1-2% lidocaine
Reponses ceases with repeated stimulation Reflex is more sensitive in neonates and children, especially during squint surgery Incidence during ophthalmic surgery: 30-90%
Reflex activated by Cerebral edema Hematoma – subdural, epidural, contusion, ICH Foreign body Depressed skull fracture Hydrocephalus Hypoventilation Venous sinus thrombosis IC-SOL: Tumor, hematoma, abscess Brainstem compression Acute traumatic brain injury Craniotomy Neuroendoscopy Cushing Reflex
CSF pressure / ICT Compression of cerebral arteries Cerebral ischemia at the medullary VMC ( CO2 in blood, lactic acid in VMC) Stimulates vasoconstrictor and cardioaccelerator neurons in VMC Sympathetic stimulation HR, BP, myocardial contractility improve cerebral perfusion Stimulaes baroreceptors Reflex bradycardia
Triad of HTN, bradycardia and apnea • Seen in 33% of patients with ICT • Inhalational agents are generally associated with ICT • Both thiopental and propofol ICT • Occurrence of bradycardia & HTN is used as warning sign of ICT during neuroendoscopy