Download
1 / 42
440 likes | 800 Views
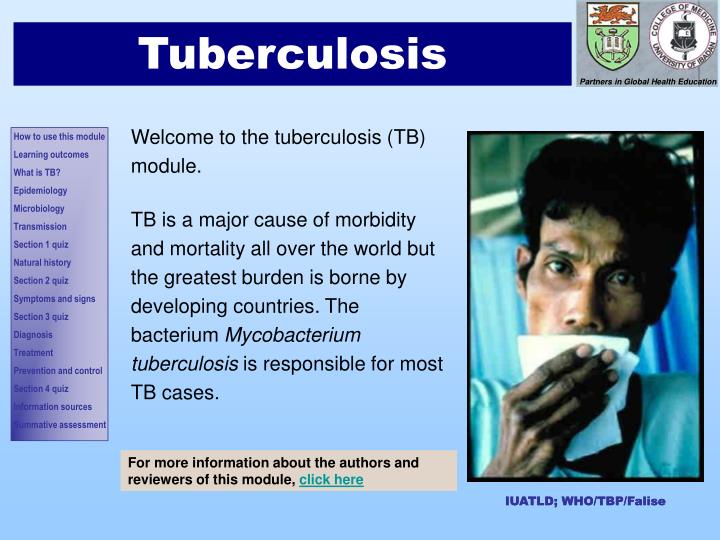
Introduction 1. Tuberculosis. Welcome to the tuberculosis (TB) module. TB is a major cause of morbidity and mortality all over the world but the greatest burden is borne by developing countries. The bacterium Mycobacterium tuberculosis is responsible for most TB cases.

E N D
Introduction 1 Tuberculosis Welcome to the tuberculosis (TB) module. TB is a major cause of morbidity and mortality all over the world but the greatest burden is borne by developing countries. The bacterium Mycobacterium tuberculosis is responsible for most TB cases. For more information about the authors and reviewers of this module, click here IUATLD; WHO/TBP/Falise IUATLD; WHO/TBP/Falise
Introduction 2 How should you study this module? • We suggest that you start with the learning objectives and try to keep these in mind as you go through the module slide by slide, in order. • Print-out the mark sheet • As you go along, write your answers to the questions on the mark sheet as best you can before looking at the answers. • Award yourself marks as detailed on the mark sheet: one mark for each keyword (shown in red text) in the short answer questions and for every correct answer in the True/False questions. • Repeat the module until you have achieved a mark of 28/35 (≥80%). • Finish with the formative multiple choice questionnaire to assess how well you have covered the material as a whole. • You should research any issues that you are unsure about. Look in your textbooks, access the on-line resources indicated at the end of the module and discuss with your peers and teachers. • Finally, enjoy your learning! We hope that this module will be enjoyable to study and complement your learning about TB from other sources.
Introduction 2 Learning Outcomes By the end of the module, you should be able to: • Describe how TB can affect anyone, of any age, anywhere, but that most cases occur in specific risk groups • Describe how respiratory droplets are the main transmission agent • Describe how, following inhalation, M. tuberculosis causes infection in many people and disease in some • Enumerate the general symptoms and signs of TB and the specific clinical features of pulmonary TB • Discuss how CXR and sputum examination are used in diagnosis • Describe how TB is managed using combinations of antimicrobials • Describe how TB is prevented at the community level by immunisation, case finding and contact tracing
What is tuberculosis (TB)? TB is a chronic bacterial infection. The great majority of infections in people are caused by Mycobacterium tuberculosis (M.tuberculosis). A closely related bacteria, M. bovis, causes TB in animals (especially cattle) and can infect people who drinkunpasteurised milk from infected cows. Although an ancient disease, TB remains a world wide problem: • about 1 in 3 of the world’s population is infected with tubercle bacilli and someone is newly infected every second • although most infected people remain asymptomatic, there are about 9 million new cases and nearly 2 million TB deaths every year.
The largest number of cases and highest mortality occur in South East Asia and this region accounts for 33% of incident cases globally. The annual incidence of TB is increasing sub-Saharan Africa mainly as a result of the increased susceptibility of people infected with HIV. Other factors which encourage TB transmission are: the emergence of multidrug-resistant strains of M. tuberculosis poor national TB control programmes and worsening socio-economic conditions in many countries In the UK, the annual incidence rate is increasing with >8,000 new cases/year. Most occur in the larger cities, especially London, and about 2/3 cases occur in people who were born abroad. TB causes or contributes to 300-400 deaths/year in the UK. Epidemiology 4 Where does TB occur? About 95% of the world’s cases of TB occur in South East Asia, sub-Saharan Africa and the Western Pacific.
Epidemiology 2 Microbiology (1) M. tuberculosis is a non-motile, rod-shaped bacterium measuring 2-4 x 0.2-0.5 μm. It is an obligate aerobe, which explains why it tends to be found in the well-aerated, upper lobes of the lungs. It is a slow growing organism (dividing only every 16-20 hours) that lives within tissue macrophages. Humans are the only reservoir of M. tuberculosis. Both animals and humans serve as reservoirs for M. bovis. The organism does not have the characteristics of either Gram positive or negative bacteria. It has a peculiar cell wall that consists of peptidoglycan and complex lipids. Once stained (e.g. with carbol fuchsin), the organism will retain dyes when treated by acidified organic compounds. Therefore, it is classified as an “acid–fast” bacterium. The Ziehl-Nielsen stain is used to demonstrate the presence of the bacilli in a smear. Note the bright red rods in this sputum smear.
Epidemiology 3 Microbiology (2) The cell wall is a major factor in the virulence of the organism. It resists destruction by many antibiotics, acids, alkalis, osmotic lysis and oxidation and enables the organism to survive and multiply within macrophages. M. tuberculosis grows in Lowenstein Jensen medium, an egg-based medium, which contains inhibitors to keep contaminants from outgrowing the organism. Because of its slow growth, it takes 4-6 weeks before small buff-coloured colonies are visible on the medium. Typical small, buff coloured colonies of M. tuberculosis on Lowenstein Jensen medium
Transmission 1 How is TB transmitted? Nearly all TB infection is acquired by inhalation of respiratory droplets from people with TB in the lungs or throat. Air droplets 3-5 μm diameter are coughed, sneezed or spat-out by an “open” case of TB. The droplets are inhaled by a close contact. This is more likely to occur in overcrowded environments. NB. Abdominal TB can also result from drinking unpasteurised cow’s milk infected with M. bovis.
End of Section 1 Well done! You have come to the end of the first section. We suggest that you answer questions 1 to assess your learning so far. Please remember to write your answers on the mark sheet before looking at the correct answers!
Question 1: Risk of exposure to TBWrite “True” or “False” on the answer sheet. When you have completed all 5 questions, click on the boxes and mark your answers. Now that you know how TB is transmitted, are the following people at increased risk of exposure? Click for the correct answer • Close contacts of people with open TB (e.g. family members) • People who drink unpasteurised milk • People living in poor, overcrowded environments • People who work or are residents in long-term facilities • Infants and young children a a a a a a a a a a b b b b b b b b b c c c c c c c d e e e
Pathogenesis 1 What happens following inhalation of M. tuberculosis?Outcome 1: No infection • Between 70-90% of individuals exposed to TB will not develop the infection. • The reasons for this are unclear. However, in view of the known risk factors for infection, people who inhale bacilli but do not develop an infection may: • inhale too few organisms to cause infection • have sufficient immunity to prevent an infection becoming established • Any factor associated with impaired immunity, such as extremes of age, malnutrition and HIV/AIDS will increase the risk of developing infection.
Pathogenesis 2 What happens following inhalation of M. tuberculosis?Outcome 2: Infection with formation of a primary complex Following inhalation, tubercle bacilli settle in the alveoli and result in local inflammation in the lung parenchyma. This “primary focus” usually occurs in the upper lobes in adults but may occur in any of the lung lobes in children. More than one focus may occur in the same patient. The organisms then spread via the local lymphatics to the nearest hilar lymph nodes, which may then enlarge. The primary focus and the enlarged regional lymph nodes form the “primary complex” or “Ghon complex”. What happens next depends on the size of the infecting dose and the resistance of the host. Most commonly, the primary focus is “walled-off” by the immune system and lies dormant– “latent TB”. The infection may be reactivated years later if the immune system of the host becomes weakened. Primary focus successfully contained by the host immune system The person is infected but does not have TB disease and cannot spread TB. However,an immune responseto M. tuberculosis will have developed – and can be demonstrated by a positive Mantoux test (see later).
If the primary focus is not contained, lung disease may develop in several ways: The primary focus enlarges and undergoes central necrosis to form a cavity The infection can spread locally and result in tuberculous bronchopneumonia Marked swelling of the mediastinal lymph nodes may compress large bronchi and result in lobar collapse The enlarged lymph node may act like a one-way valve causing hyperinflation of a lung or lobe The adjacent pleura can become infiltrated by M. tuberculosis resulting in a hypersensitivity reaction characterised by granulomas composed mainly of lymphocytes Pleural infiltration may result in a pleural effusion which is rich in lymphocytes – a useful pointer to the diagnosis when pleural fluid is aspirated and analysed Long term complications of the damage to lung tissue include emphysema and bronchiectasis What happens following inhalation of M. tuberculosis?Outcome 3: Pulmonary disease Pathogenesis 3 Infection not contained by the immune system. Person develops lung disease and becomes an open case - capable of infecting others via respiratory droplets.
Pathogenesis 4 What happens following inhalation of M. tuberculosis?Outcome 4: Systemic disease Haematogenous dissemination of M. tuberculosis leads to granuloma formation in many organs. Examples include: • Diffuse infection of the lungs: “miliary” TB • Brain: TB brain abscess • Meninges: TB meningitis • Bones: TB osteomyelitis – commonly affects the spine and is then called “Potts’ disease” • Pericardium: TB pericarditis and pericardial effusion As with acquiring infection after inhalation, disseminated disease is most likely to occur in the immunocompromised person (e.g. HIV/AIDS, malnutrition) and at extremes of age.
Summary (1): natural history following TB exposure Pathogenesis 5 What are the likely outcomes following exposure to open TB? Exposure to TB Infection (10-30%) No infection (70-90%) • Active TB (10%) • ill and likely to die if untreated • infectious • Dormant TB (90%) • well • no TB disease • not infectious to others Activation of infection results in disease
Pathogenesis 1 Summary (2): natural history following TB exposure There are 4 possible outcomes following inhalation of TB bacilli: Note: outcomes 3 and 4 can develop many years after formation of the 1o lung complex
End of Section 2 Well done! You have come to the end of the second section. Answer questions 2 through 4 to assess your learning so far. Challenge yourself: complete the mark sheet before looking at the correct answers!
Question 2: Groups of people at increased risk of TB disease and disseminated infection following exposure are:Write “True” or “False” on the answer sheet. Click for the correct answer • Infants and children <5 years • People with HIV/AIDS • People with diabetes mellitus, measles, pertussis or on prolonged corticosteroid therapy • Young adults • Alcoholics and IV drug users a b c d e
Question 3: Factors underlying the resurgence of TB in the last 2 decades are:Write “True” or “False” on the answer sheet. Click for the correct answer • HIV pandemic • Poverty/worsening socioeconomic conditions • Poor hygiene • Emergence of drug resistance strains • Poor national TB control programmes a b c d e
Question 4: Following exposure to M. tuberculosis Write “True” or “False” on the answer sheet. Click for the correct answer • The usual outcome is a primary infection • The primary complex consists of a cavity in the lung parenchyma and hilar lymphadenopathy • A pleural aspirate rich in neutrophils suggests TB as a cause • Miliary TB refers to disseminated infection spread via the bloodstream a b c d
Clinical features 1 What are the symptoms and signs of TB? 1. Primary infection with no spread of the disease • Individuals with primary infection do not usually have any symptoms or signs of ill health although some people develop a minor flu-like illness. • Infection triggers an immune response and, in aminority of people, this may result in clinical signs of hypersensitivity to M. tuberculosis for example: • erythema nodosum • phlyctenular keratoconjunctivitis • They will also have a positive Mantoux test (see below). Erythema nodosum: ecchymotic papules found along the shin or on the flexural surfaces of the limbs Phlyctenular keratoconjunctivitis: raised, yellowish nodule at the corneoscleral junction. Small blood vessels may be seen radiating from the nodule.
Organ specific - examples include: Lungs Cough – usually chronic (lasting >6 weeks) Productive of whitish or mucoid sputum in adults but usually unproductive in children Haemoptysis (coughing-up blood) Central Nervous System TB meningitis Tuberculoma, with the classical features of a space-occupying lesion simulating a brain tumour What are the symptoms and signs of TB? 2. Active infection: symptoms Clinical features 2 Symptoms of TBcan be divided into general symptoms and those specific to the organ infected. TB can result in a myriad of symptoms depending on which organs are involved and how their function is affected. The lung is the predominant organ affected, being involved in over 75% of cases. Commonly affected organs following haematogenous spread from the lung are the abdomen, lymph nodes, spine, meninges, kidneys, bone and reproductive organs. • General symptoms • Fever • Loss of weight in adults or growth faltering in children • Night sweats • Malaise, tiredness and anorexia
Clinical features 3 What are the symptoms and signs of TB? 2. Active infection: signs • General examination - look for: • fever • signs of malnutrition signifying a chronic illness • enlargement of the peripheral lymph nodes • digital clubbing as a consequence of chronic infection/inflammation in the chest or abdomen TB lymphadenitis presents as painless enlargement of the superficial lymph nodes. The neck is the commonest site involving the cervical, submandibular, pre and post-auricular lymph nodes. The lymph nodes are non-tender, matted together and rubbery in consistency. It is common for enlarged lymph nodes to ulcerate and discharge. Look at this picture of a 4 year old boy from West Africa. Note that he is generally wasted and has marked enlargement of the cervical lymph nodes – especially on the right side.
Clinical features 3 What are the symptoms and signs of TB? 3. Pulmonary and abdominal TB Pulmonary TB (PTB) The apical region is the most commonly affected in adults. Pulmonary lesions may involve any part of the lung in infancy and childhood. Abnormalities detected clinically include consolidation, collapse, pleural effusion and fibrosis. But beware: examination of the respiratory system may be completely normal even in active disease! Upper lobe changes on CXR Source: WHO/TBP/Pierre Virot Abdominal TB Pathology affects the mesenteric and the retroperitoneal glands, the omentum and the gastrointestinal tract. Patients may present with weight loss, diarrhoea or constipation, abdominal distension (from ascites) or chronic intestinal obstruction. Enlarged mesenteric lymph nodes may be palpable as multiple intra-abdominal masses.
Tuberculosis of the spine – “Pott’s disease” TB commonly affects the spine, especially in young children, and usually presents as a swelling on the back. The lower thoracic and the upper lumbar vertebrae are the usual sites, however any vertebra can be affected. The patient may also present with kyphosis, scoliosis, kyphoscoliosis, or features of spastic paraparesis. There may be a sharp angulation of the spine caused by collapse of a vertebra – referred to as a “gibbus” A young child from West Africa. Note the swelling over the lower thoracic vertebrae.
End of Section 3 Well done! This is the end of the second section. We suggest that you proceed to answer question 5 to assess your learning further. Do remember to write your answers on the mark sheet before looking at the right answer!
Clinical features Quiz 1 Question 5: What 2 features are consistent with pulmonary TB in this man? Write Down Your Answers on your mark sheet, then click below to reveal the answers Man with advanced TB in Bangladesh source: WHO/TBP/England Click to Reveal Answers
Investigation 1 Diagnosis In developing countries, the diagnosis of TB is based on the combination of clinical assessment and simple laboratory methods: • History of chronic cough with the general symptoms of fever, malaise and weight loss • Presence of general and specific clinical signs • Positive findings on relevant investigations – usually CXR and sputum smear stained for acid-fast bacilli It is important to note that specific symptoms and signs may be absent. Examining a CXR in China Source: WHO/TBP/Pierre Virot TBshould be suspected in any chronically ill person!
Investigation 4 Bacteriological diagnosis • Sputum microscopy is most useful in adults with a productive cough. A sputum smear is stained with the Ziehl-Nielsen stain to demonstrate the presence of the acid and alcohol fast bacilli (AFB). When positive, the patient is “smear-positive” or “open TB” and the risk of transmission of infection to others is very high. However, the test is often falsely negative in patients with TB. The yield of the test is higher in patients with lung cavities. • Gastric washings examined for AFB: Carried out in children as they swallow rather than cough-up sputum. The test aims to recover the swallowed AFB from the stomach using a naso-gastric tube. The test is positive in only about one third of children with TB. • Bacterial culture: This takes about 6-8 weeks and so is of limited use in clinical diagnosis. M. tuberculosis grows on a special medium called the Lowenstein Jensen medium. Sputum samples collected in a health facility in Ethiopia source: WHO/TBP/Jan Van den Hombergh
Investigation 5 Mantoux or tuberculin skin test This test detects a delayed hypersensitivity, cutaneous reaction to a purified protein derivative (PPD) of M. tuberculosis – also called “tuberculoprotein”: • PPD is injected intradermally • the injection site is inspected 48-72 hours later • erythema and induration at the site signify an immune response and, therefore, previous exposure to mycobacteria The limitations of this test are well-known: • False positive: a skin reaction in people who do not have TB because of exposure to non-pathogenic mycobacteria and also due to the immune response following BCG immunisation (see later). • False negative: a negative result in a person with TB in early primary infection or because they are immunocompromised – for example, due to HIV/AIDS, malnutrition or people who develop disseminated TB. In general, the greater the degree of erythema and induration, the more likely the patient has TB disease. Several detailed criteria are available to guide the interpretation of Mantoux results, e.g. from the American Thoracic Society and Centers for Disease Control & Prevention
Investigation 7 Diagnosis: Other investigations Other investigations are indicated depending on the organs/ systems affected by the disease • Spinal radiographs in Pott’s disease • Lymph node aspirate (microscopy, culture and cytology) or biopsy (histology and culture) in TB lymphadenitis • Lumbar puncture for cerebrospinal fluid analysis in TB meningitis (microscopy, biochemical analysis and culture) A recent development is the detection of the growth of TB in liquid culture by microscopy. Diagnosis can be made within 10 days and addition of drugs to the cultures allows the detection of drug resistance.* Also, a number of new diagnostic tests have been developed based on molecular methods such as the amplification of nucleic-acid. However, these assays have not been fully evaluated and are expensive. * Moore DA et al. Microscopic-observation drug-susceptibility assay for the diagnosis of TB. N Engl J Med 2006; 355:1539-50
Treatment Resistance of M. tuberculosis to antimicrobials is a major problem in TB treatment. Because it is a slow growing organism, treatment courses are long - at least 6 months. • Treatment requires a combination ofdrugs to which the organisms are sensitive. • Treatment courses must be completed for effective cure and to prevent the emergence of drug-resistant strains. • Longer treatment courses are needed for TB meningitis or if the bacteria are resistant and additional drugs are required. Combination antibiotic therapy in India Source: IUTBLD WHO/TBP/Gary Hampton
Management Treatment: DOTS • DOTS is the acronym for Directly Observed Treatment Short Course. • It involves the daily administration of a combination of antituberculous drugs to a TB patient under the supervision of a healthcare personnel. DOTS helps to ensure compliance, reduce transmission by shortening the period of infectivity, improve the cure rate and reduce the risk of drug resistance. • There are many regimens for treating TB. The most frequently recommended regimen that is also effective in people with HIV infection is: • *IM streptomycin is often substituted for oral ethambutol for children < 6 years
Drug-resistant TB There are 2 classes of drug resistant TB: 1. Multidrug-resistant (MDR) • defined as resistance to rifampicin and isoniazid, +/- other drug resistance • worldwide, >4% of TB patients are MDR, with the highest prevalence in Eastern Europe • treatment requires longer drug regimens, is less effective, more costly and poorly tolerated 2. Extensively drug-resistant (XDR) • defined as resistance to rifampicin and isoniazid and, in addition, resistance to any quinolone and at least on injectable second-line drug • XDR TB is essentially untreatable and has a very high mortality
Prevention Prevention and Control TB control strategies include – • Case finding: aims to identify TB cases promptly, treat them with an effective combination of drugs and ensure that the course is completed. • Contact tracing: Close contacts of TB cases are screened for evidence of infection. Mantoux positive cases are treated with oral isoniazid for 6-12 months to prevent them from developing the disease. This regimen is also used in HIV-positive people. • Bacillus Calmette-Guérin (BCG)vaccine • contains an attenuated strain of M. bovis • is administered as a single intradermal injection • Has limited efficacy against pulmonary TB (and, therefore, TB transmission) but does appear to prevent disseminated disease and death – especially in children • is given routinely to infants in developing countries and to people at increased risk of TB infection in developed countries
TB: the future WHO declared TB a global health emergency in 1993 and aims to eliminate TB as a public health problem by 2050. • Other organisations involved in TB control include the International Union Against TB and Lung Disease, the Center for Disease Control (USA) and the Global Plan to Stop TB. • TB remains a worldwide challenge. There is a need to improve DOTS coverage and meet the emerging challenges of TB in people with HIV/AIDS and multidrug resistant TB. • Improved techniques for diagnosis are required especially in people with compromised immunity where diagnosis is difficult such as HIV/AIDS and malnourished children. • A more effective vaccine and improved treatment strategies that would decrease the duration of treatment are also high priorities. IUATLD; WHO/TBP/Falise
End of Section 4 You have come a long way! This is the last of the sections. For the section just ended, you should be able to answer Questions 6 - 8 to assess what you have learnt. It is still required that you put down your answers on the mark sheet before looking at the right answer!
Question 6: A person with latent TBWrite “True” or “False” on the answer sheet. Click for the correct answer • Is infectious to other people • Feels well • Tuberculin skin test is positive • Can not develop TB later in life a b c d
Question 7: The following are recognised manifestations of TB Click for the correct answer • Pericarditis • Meningitis • Erythema nodosum • Osteomyelitis • Phlyctenular conjunctivitis a b c d e
Question 8: The following are indicated in the management of miliary TB Click for the correct answer • High protein diet • BCG Vaccination • Contact tracing • Isoniazid prophylaxis for 6-12 months • Lumbar puncture a b c d e
Sources of information / bibliography You can copy and paste the links below into your browser to access the resources: • Maartens G, Wilkinson RJ. Tuberculosis. The Lancet 2007; 370:2030-43 • Diagnostic atlas of intra-thoracic tuberculosis in children; A guide for Low Income Countries. Dr. Robert Gie, International Union against Tuberculosis and Lung Disease (IUATLD) 2003. Available at: http://www.iuatld.org • The Division for Tuberculosis Elimination, Centre for Disease Control (CDC), Atlanta, USA http://www.cdc.gov/nchstp/tb/faqs/qa.htm • Stop TB Partnership; http://www.stoptb.org/ • WHO – several information resources available at http://www.who.int/tb/en/ • Treatment guidelines: http://www.Nice.ac.uk • TB in the UK: http://www.Hpa.org.uk
Summative assessment • Well done! We hope that you enjoyed completing this module. • Now try the summative assessment (available fromhttp://www.medicine.swansea.ac.uk/inthealth.html) • … and good luck!