Download

1 / 48
510 likes | 818 Views
ARDS. g.k.kumar. ARDS. Definition Epidemiology Patient presentation and diagnosis Pathophysiology Treatment Complications. Historical background First described in 1967 by Ashbaugh et al Consensus after 1994

E N D
ARDS g.k.kumar
ARDS • Definition • Epidemiology • Patient presentation and diagnosis • Pathophysiology • Treatment • Complications
Historical background • First described in 1967 by Ashbaugh et al Consensus after 1994 • In 1994 a new definition was recommended by the American-European Consensus Conference Committee.
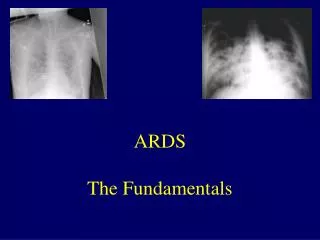
Definition ARDS is characterized by • Acute onset • Bilateral infiltrates on chest radiograph • Pulmonary artery wedge pressure < 18 mmHg; if unavailable, then lack of clinical evidence of left ventricular failure suffices • PaO2:FiO2 < 200 mmHg
Epidemiology • The annual incidence of ARDS 1.5 to 13.5 people per 100,000 in the general population. In mechanically ventilated population is much higher. • (ALI) of 16.1% in ventilated patients admitted for more than 4 hours. • More than half these patients may develop ARDS - Brun-Buisson et al. (2004)
Risk factors • Mechanical ventilation, sepsis, pneumonia, shock, aspiration, trauma (especially pulmonary contusion), major surgery, massive transfusions, smoke inhalation, drug reaction or overdose, fat emboli and reperfusion pulmonary edema after lung transplantation or pulmonary embolectomy. Pneumonia and sepsis are the most common triggers, and pneumonia is present in up to 60% of patients. • Elevated abdominal pressure of any cause is also probably a risk factor for the development of ARDS, particularly during mechanical ventilation.
Predisposing Factors Pulmonary conditions • Severe pneumonia. • Aspiration • Near drowning. • Inhalation of toxins and other irritants such as smoke. • Lung injury and bruising. • Oxygen toxicity. • Fat embolism- Where bubbles of fat travel through the bloodstream and block off airways.
Predisposing Factors Systemic conditions • Shock- Including septic shock and shock due to trauma. • Septicaemia. • Burns. • Pancreatitis. • Diabetic Ketoacidosis. • Hypersensitivity reactions. • Drugs reactions due to aspirin, heroin or paraquat. • Multiple blood transfusions. • Malaria. • Acute liver failure. • Obstetric complications- Problems during pregnancy or delivery such as preeclampsia. • Cardiac surgery and other complicated surgeries.
Patient presentation and diagnosis • ARDS usually occurs within 24 to 48 hours of the initial injury or illness. • The patient usually presents with shortness of breath, tachypnea, and symptoms related to the underlying cause, i.e. shock
Patient presentation and diagnosis • Arterial blood gas analysis • Chest X-ray • Pulmonary artery catheter for measuring the pulmonary artery wedge pressure. • CT scanning
Pathophysiology • Diffuse inflammation of lung parenchyma • Typical histological presentation involves diffuse alveolar damage and hyaline membrane formation in alveolar walls.
Pathophysiology • Endothelial dysfunction, fluid extravasation from the capillariesand impaired drainage of fluid from the lungs. • This pulmonary edema increases the thickness of the alveolo-capillary space. • This impairs gas exchange leading to hypoxia, increases the work of breathing, eventually induces fibrosis of the airspace.
Pathophysiology • Dysfunction of type II pulmonary epithelial cells, with a concomitant reduction in surfactant production. • Edema and decreased surfactant production by type II pneumocytes may cause whole alveoli to collapse, or to completely flood.
Pathophysiology • This loss of aeration contributes further to the right-to-left shunt, resulting in massive intrapulmonary shunting. • The loss of aeration may follow different patterns according to the nature of the underlying disease, and other factors
Pathophysiology • In pneumonia-induced ARDS, infiltrates are usually distributed to the lower lobes, in their posterior segments, and they roughly correspond to the initial infected area.
Pathophysiology • In sepsis or trauma-induced ARDS, infiltrates are usually more patchy and diffuse. The posterior and basal segments are always more affected, but the distribution is even less homogeneous.
Treatment • Mechanical ventilation • Antibiotic • When sepsis is diagnosed, appropriate protocols should be enacted.
Mechanical ventilation • The overall goal is to maintain acceptable gas exchange and to minimize adverse effects in its application. • Three parameters are used: PEEP, to maintain maximal recruitment of alveolar units. Mean airway pressure (to promote recruitment and predictor of hemodynamic effects) Plateau pressure (best predictor of alveolar overdistention).
Mechanical ventilation • Low tidal volume ventilation • Plateau pressure less than 30 cm H2O was a secondary goal, • APRVis the primary mode of choice when ventilating a patient with ARDS or ALI.
AIRWAY PRESSURE RELEASE VENTILATION(APRV) • A CPAP circuit with release valve at expiratory limb –driven by time device • APRV is a CPAP system causing . alveolar ventilation by briefly interrupting CPAP.
APRV • Release valve opens for 1-2sec. • Pr drops to lower level-low CPAP(0to-2cmH2O) • Lung volume less than FRC in expiration • alveolar ventilation & CO2 elimination • Reapplication of CPAP by closing valve- Higher CPAP(10to 12 cm H2O) • FRC & oxygenation.
APRV • ADVANTAGES: • Lesser PIP ,so less hemo dynamic changes. • To alveolar ventilation in ALI of mild to moderate. • A weaning mode.
Mechanical ventilation Advantages to APRV ventilation • decreased airway pressures, • decreased minute ventilation, • decreased dead-space ventilation, • promotion of spontaneous breathing, near elimination of neuromuscular blockade • almost 24 hour a day alveolar recruitment, • decreased use of sedation, • positive effect on cardiac output (due to the negative inflection from the elevated baseline with each spontaneous breath). • A patient with ARDS on average spends 8 to 11 days on a mechanical ventilator; APRV may reduce this time significantly.
INVERSE RATIO VENTILATION(IRV) • I:E >1 • PC-IRV / VC-IRV • Ti with set pr opening of stiff alveoli units improved oxygenation • Te not allowing alveoli to collapse • development of intrinsic PEEP • reduction of shunting
IRV……, • Improve oxygenation by • Reducing intra pulmonary shunting • Improvement of V/Q matching • Decreased dead space ventilation • Increased MAP & intrinsic PEEP • Useful when high FiO2 & high PEEP to be avoided
Inverse ratio ventilation • Inverse ratio ventilation is reserved for severe cases when it is impossible to oxygenate the patient adequately. • Treatment involves increasing the amount of time that the ventilator is inspiring versus expiring. • Patients normally spend more time exhaling than inhaling, at a ratio of about 3:1. Increasing the amount of time spent inhaling re-expands more collapsed alveoli than positive pressure alone. • This is an uncomfortable technique and usually requires sedation and a muscle-paralyzing drug that keeps the respiratory muscles from resisting the unnatural inverse ratio ventilation.
Prone position ventilation • Distribution of lung infiltrates in acute respiratory distress syndrome is non-uniform. • Repositioning into the prone position (face down) might improve oxygenation by relieving atelectasis and improving perfusion.
Prone position ventilation • Improved V/P in previously atelectactic areas due to uniform distribution of plural pr -Lamm etall • Requires atleast more than 6 hrs/ day of prone ventilation. • A significant decrease in right ventricular enlargement and a significant reduction in septal dyskinesia, after 18 h of prone positioning.-Vielliard etall ,CHEST-OCT-2007 • No improvement in mortality in clinical trials
Fluid management • Several studies have shown that pulmonary function and outcome are better in patients that lost weight or wedge pressure was lowered by diuresis or fluid restriction
Corticosteroid • Steroids cause a suppression of inflammation during the fibroproliferative phase of ARDS. The initial regimen consists of mps 2 mg/kg daily. After 3-5 days a response must be apparent. In 1-2 weeks the dose can be tapered to mps 0.5-1.0 mg daily. In the absence of results steroids can be discontinued.-Meduri et al • ARDSnet LAZARUS study demonstrated that they are not efficacious in ARDS.
Nitric oxide • Inhaled nitric oxide (NO) potentially acts as selective pulmonary vasodilator. Rapid binding to hemoglobin prevents systemic effects. It should increase perfusion of better ventilated areas. There are no large studies demonstrating positive results. • Almitrine bismesylate stimulates chemoreceptors in carotic and aortic bodies. It has been used to potentiate the effect of NO, presumably by potentiating hypoxia-induced pulmonary vasoconstriction. In case of ARDS it is not known whether this combination is useful.
Surfactant therapy • To date no prospective controlled clinical trial has shown a significant mortality benefit of exogenous surfactant in ARDS • IV N-Acetyl-Cysteine which may increase the lung surfactants
Anti-inflammatory Strategies • Antioxidant Therapy -N-acetylcysteine and procysteine, oxygen free-radical scavengers and precursors for glutathione, were efficacious in some experimental studies • Prostaglandin Agonists/Inhibitors: Prostaglandin E1 is a vasodilator that blocks platelet aggregation and decreases neutrophil activation • Ibuprofen- an inhibitor of the cyclooxygenase pathway • Ketoconazole, a potent inhibitor of thromboxane and leukotriene synthesis • Pentoxifylline is a phosphodiesterase inhibitor that inhibits neutrophil chemotaxis and activation in animal models of ARDS • Lisofyllineinhibited release of TNF, IL-1, and IL-6, • Anti–IL-8 Therapy
Enhanced Resolution of Alveolar Edema Alveolar fluid clearance depends primarily on active sodium transport across the alveolar epithelium • Salmeterol, a lipid-soluble ß2-agonist • Intra-alveolar terbutaline administration markedly increased alveolar fluid clearance • Dobutamine, ß2-adrenergic agonist, markedly increased alveolar and lung fluid clearance in an experimental rat model • Dopamine, when administered at 5 µg/kg/min IV, increased alveolar fluid clearance in an isolated perfused rat model by increasing the activity of . Na-K ATP pumps.
Enhanced Repair of the Alveolar Epithelial Barrier • Studies suggest that hepatocyte growth factor and keratinocyte growth factor are major mitogens for alveolar epithelial type II cells
Complications • Pulmonary: barotrauma (volutrauma), pulmonary embolism (PE), pulmonary fibrosis, ventilator-associated pneumonia (VAP). • Gastrointestinal: hemorrhage (ulcer), dysmotility, pneumoperitoneum, bacterial translocation. • Cardiac: arrhytmias, myocardial dysfunction. • Renal: acute renal failure (ARF), positive fluid balance.
Complications • Mechanical: vascular injury, pneumothorax (by placing pulmonary artery catheter), tracheal injury/stenosis (result of intubation and/or irritation by endotracheal tube. • Nutritional: malnutrition (katabolic state), electrolyte deficiency.
ARDS Dr.G.K.Kumar