Download
1 / 27
270 likes | 523 Views
University of Oklahoma School of Community Medicine Department of Family Medicine Presented By: Frances Wen, PhD January 26, 2010. Every Doc Can Write An Abstract & Do A Case Report. Abstracts. What is it? Why are they used?

E N D
University of Oklahoma School of Community Medicine Department of Family Medicine Presented By: Frances Wen, PhD January 26, 2010 Every Doc Can Write An Abstract & Do A Case Report
Abstracts • What is it? • Why are they used? • OU Health Research Forum and OUFM Department Research Day abstracts are due Feb. 15, 2010 • Format used? • Refer to “Call for abstracts notification”—usually lists format required and a limitation of 400 words. http://library.tulsa.ou.edu/ocs/index.php/testconference/2010/schedConf/cfp
Basic Components of An Abstract • Introduction • Why do we care about the problem? • What practical, scientific gap is your research filling? • Methods • What did you do to get your results • Results • What did you learn? • Conclusions • What are the larger implications for your findings, especially for the problem/gap identified in the Introduction?
Abstract Criteria • Hypothesis/purpose/objective of research clearly stated • Methods and materials essential to the research identified • Study design, sampling, sample size, procedures, power analysis, data analysis, limitations • Results, or predicted results clearly represented and logically support proposed or predicted conclusions • Analytic procedures used are clear; data linked to study purpose • Scientific merit and future directions of the research • Well developed writing skills
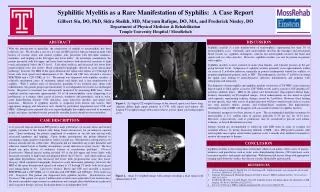
Osteopathic manipulative treatment and its relationship to autonomic nervous system activity as demonstrated by heart rate variability: a repeated measures study Charles E Henley, Douglas Ivins, Miriam Mills, Frances K Wen and Bruce A Benjamin Osteopathic Medicine and Primary Care 2008, 2:7 Background: The relationship between osteopathic manipulative treatment (OMT) and the autonomic nervous system has long been acknowledged, but is poorly understood. In an effort to define this relationship, cervical myofascial release was used as the OMT technique with heart rate variability (HRV) as a surrogate for autonomic activity. This study quantifies that relationship and demonstrates a cause and effect. Methods: Seventeen healthy subjects, nine males and eight females aged 19–50 years from the faculty, staff, and students at Oklahoma State University Center for Health Sciences College of Osteopathic Medicine, acted as their own controls and received interventions, administered in separate sessions at least 24 hours apart, of cervical myofascial OMT, touch-only sham OMT, and no-touch control while at a 50-degree head-up tilt. Each group was dichotomized into extremes of autonomic activity using a tilt table. Comparisons were made between measurements taken at tilt and those taken at pre- and post-intervention in the horizontal. The variance of the spectral components of HRV, expressed as frequencies, measured the response to change in position of the subjects. Normalized low frequency (LF) and high frequency (HF) values, including LF/HF ratio, were calculated and used to determine the effect of position change on HRV. Results: Predominantly parasympathetic responses were observed with subjects in the horizontal position, while a 50-degree tilt provided a significantly different measure of maximum sympathetic tone (p < 0.001). Heart rate changed in all subjects with change in position; respirations remained constant. When OMT was performed in a sympathetic environment (tilt), a vagal response was produced that was strong enough to overcome the sympathetic tone. There was no HRV difference between sham and control in either the horizontal or tilt positions. Conclusion: The vagal response produced by the myofascial release procedure in the maximally stimulated sympathetic environment could only have come from the application of the OMT. This demonstrates the association between OMT and the autonomic nervous system. The lack of significance between control and sham in all positions indicates that HRV may be a useful method of developing sham controls in future studies of OMT.
Background: The relationship between osteopathic manipulative treatment (OMT) and the autonomic nervous system has long been acknowledged, but is poorly understood. In an effort to define this relationship, cervical myofascial release was used as the OMT technique with heart rate variability (HRV) as a surrogate for autonomic activity. This study quantifies that relationship and demonstrates a cause and effect.
Methods: Seventeen healthy subjects, nine males and eight females aged 19–50 years from the faculty, staff, and students at Oklahoma State University Center for Health Sciences College of Osteopathic Medicine, acted as their own controls and received interventions, administered in separate sessions at least 24 hours apart, of cervical myofascial OMT, touch-only sham OMT, and no-touch control while at a 50-degree head-up tilt. Each group was dichotomized into extremes of autonomic activity using a tilt table. Comparisons were made between measurements taken at tilt and those taken at pre- and post-intervention in the horizontal. The variance of the spectral components of HRV, expressed as frequencies, measured the response to change in position of the subjects. Normalized low frequency (LF) and high frequency (HF) values, including LF/HF ratio, were calculated and used to determine the effect of position change on HRV.
Results: Predominantly parasympathetic responses were observed with subjects in the horizontal position, while a 50-degree tilt provided a significantly different measure of maximum sympathetic tone (p < 0.001). Heart rate changed in all subjects with change in position; respirations remained constant. When OMT was performed in a sympathetic environment (tilt), a vagal response was produced that was strong enough to overcome the sympathetic tone. There was no HRV difference between sham and control in either the horizontal or tilt positions.
Conclusion: The vagal response produced by the myofascial release procedure in the maximally stimulated sympathetic environment could only have come from the application of the OMT. This demonstrates the association between OMT and the autonomic nervous system. The lack of significance between control and sham in all positions indicates that HRV may be a useful method of developing sham controls in future studies of OMT.
Points to Remember: • Follow format requirements • Simple language • Logical structure • Accurate • “Mini essay” of key concepts • Understandable to “others” • Proofread
Points to Remember: • Avoid abbreviations and acronyms • Do not include general introductory matters • No tables, charts • No citations, references
Case Reports • What is a case report? • Why do it?
Workbook: Case Report STEP #1 Choose Your Topic Carefully • Begin by asking, “What do I have to say”? • Is the paper worth writing? • Determine which category of case reports your project falls into. • Determine the appropriate audience and journal
Types of Case Reports • Unique, previously undescribed syndrome or disease • Unexpected association of disease that may represent a causal relationship • An important variation from an expected pattern. • Unexpected evolution suggesting a therapeutic or adverse drug reaction.
Other Types of Cases • The “Everyone Should Remember” case • The “Grand Rounds” case • The “ I –Am- Clever” case • The Goodness! “Book of Medical World Records” case
Workbook: Case Report STEP #2 Hit the Library (Lit Search)
Workbook: Case Report STEP #3 Justify Your Topic • Based on your literature search, evaluate your initial question. • Key question for scholarly case reports: • Is the topic you are reviewing unique, or has it been “beaten to death” already in the literature? • How does your topic add to what already exists?
Workbook: Case Report STEP #4 Look At What Resources Are Needed To Complete This Project • Time- Time is required to complete any project. You have to pick a narrow enough topic that you can succinctly write about. • Reviewers- (This is optional but preferred) Find a person in your clinic or hospital that can give you an honest appraisal and feedback on your paper before submitting it for publication
Workbook: Case Report STEP #5 Refine the Topic • Restate the topic in a refined form that can be tackled with available resources.
Workbook: Case Report STEP #6 Begin Writing • Introduction • Case • Discussion • Conclusion
Workbook: Case Report STEP #7 Stop Writing • After you have finished your first draft set it aside for a few weeks before beginning critical revision.
Workbook: Case Report STEP #8 Begin Review A 5-Part Review • Initial review • Organizational review • Grammar review • Style review • Readability review
Workbook Case Report STEP #9 Submit Manuscript Remember Prepare • Information for the authors section • Manuscript • Cover letters • Any other forms necessary
Workbook: Case Report STEP # 10 Sit Back and Relax
Example of an Abstract EVALUATING PRESCRIBING PRACTICES FOR UPPER RESPIRATORY TRACT INFECTION AT OU FAMILY MEDICINE Michele Bucholtz, D.O., Ph.D., Clifford Alprin, M.D., Yinyin Devoe, M.D., Hooman Tahmooreszadeh, M.D., John Tipton, M.D. The University of Oklahoma College of Medicine, Tulsa Department of Family Medicine INTRODUCTION Upper respiratory tract infections (URI) account for over 80 million office visits annually, 90% of these visits are to primary care physicians. In the past several years numerous studies have been published that show a widespread use of antibiotics for the treatment of viral URI with prescription rates for URI between 40 and 60%. Evidence from Medicaid suggests that antibiotics used to treat colds account for 23% of the total cost of managing URI and add more than $11 to the cost of managing every URI episode. This study was derived from a Pay for Performance Quality Measure proposed by the Centers for Medicare and Medicaid Services to investigate the percentage of patients with URI who were treated with antibiotics at the University of Oklahoma College of Medicine, Tulsa, Department of Family Medicine (OUFM). METHODS For this retrospective study, URI is defined as an acute, self-limiting viral infection of the upper respiratory tract. This study looked at both OUFM pediatric (ages 1-17) and adult (ages 18-100) patient populations diagnosed with acute nasopharyngitis or acute URI of multiple or unspecified sites (ICD-9 code 460 and 465 respectively). The following data was collected from the OUFM electronic medical records (EMR): gender, ethnicity, payer source, age, diagnosis, indication for treatment and whether an antibiotic was prescribed Because antibiotic therapy is shown to be effective for a variety of secondary diagnoses, the following were excluded from this study: nonsuppurative otitis media, suppurative otitis media, acute sinusitis, chronic sinusitis, acute pharyngitis, acute tonsillitis, streptococcal sore throat, pneumonia, emphysema and chronic bronchitis. RESULTS Of the 400 charts reviewed, only 377 patients fulfilled our inclusion criteria; 183 (48.5%) pediatric and 194 (51.5%) adult patients. A total of 31 patients (8%) were prescribed antibiotics, 13 (41.9%) were pediatric patients and 18 (58.1%) were adult patients. CONCLUSION We found a large difference in the OUFM prescribing practices for antibiotic treatment of URI compared to the 40 to 60% reported in other studies. This difference could be because studies have shown the further a physician is from medical school training the more likely he/she is to prescribe antibiotics for URI, and the majority of OUFM physicians are residents who have recently graduated from medical school.
Example of an Abstract PHARYNGITIS TREATMENT PATTERN AT THE OU-TULSA FAMILY MEDICINE CLINIC Raman Seth, M.D.; Garrett Sullivan, M.D.; Chris Unterseher, M.D.; Soheil Zargar, M.D.; Doug Ivins, M.D. The University of Oklahoma College of Medicine, Tulsa Department of Family Medicine INTRODUCTION To highlight concern for increased antibiotic resistance produced by physicians’ practice, a Pay for Performance Quality Measure has been proposed by the Centers for Medicare and Medicaid Services to look at physician treatment patterns, especially as they relate to pharyngitis, one of the most common chief complaints of patients treated by physicians in the U.S. Most cases are viral in nature, but regardless of the infective agent, all remain largely self-limited, rarely producing significant sequelae. Per previous studies, Group A streptococcus is the most common bacterial cause of acute pharyngitis documented in only 5-26% of cases, yet nearly 75% of patients are prescribed antibiotics for their complaint. Controversy currently exists over competing pharyngitis management strategies that emphasize patient symptom relief on one hand while prioritizing prevention of inappropriate antibiotic use on the other. The purpose of our study is to clarify how we as clinicians at the University of Oklahoma, Family Medicine Clinic (OUFM) treat our patients presenting with pharyngitis. METHODS We conducted a retrospective observational study using 254 electronic medical records of OUFM adult patients who were diagnosed with pharyngitis (ICD-9 code 462, 472.1 & 034.0) between July 2006 and July 2007. Data was collected on how many were treated with antibiotics, and of these, how we supported this decision: by rapid strep or culture results, comorbidity, or clinical grounds alone. We also analyzed our data by gender, ethnicity, payer source and age. RESULTS Of the 254 cases of pharyngitis, 136 (54%) were treated with antibiotics. Of medicated patients, 98 (72%) had rapid strep testing (RST) or culture performed: 58 (59%) showed positive results, 40 (41%) showed negative. Of those with negative results, 11 (28%) had an alternative diagnosis (e.g. sinusitis or bronchitis) supporting antibiotic use, while the remaining 29 (72%) were given antibiotics solely from clinical judgment. Of the 38 patients who received antibiotic treatment without RST or culture performed, 10 had an alternative diagnosis and 28 had clinical judgment supporting the prescription. CONCLUSION While still having room to improve, it does appear clinicians at OUFM are sensitive to the issue of increasing antibiotic resistance caused by inappropriate antibiotic use. Our antibiotic prescribing pattern in adults presenting with pharyngitis appears more judicious as compared with other published studies. In the future, by expanding analysis to include the prescribing pattern in our pediatric population as well, a more complete representation may be possible.
Example of an Abstract OU FAMILY MEDICINE TREATMENT OF CARDIOVASCULAR DISEASE IN DIABETICS Ron Gann, D.O.; Heather Cribbs, D.O.; Sandra Hutchison, M.D.; Jon Ference, Pharm.D. University of Oklahoma College of Medicine, Tulsa Department of Family Medicine INTRODUCTION The American Diabetes Association’s (ADA) present recommendations are made for the treatment of blood pressure in diabetics to maintain systolic pressure <130 mmHg and diastolic <80 mmHg with either angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB), if tolerated by the patient. Recommendations for low density lipoprotein (LDL) were also made to keep the level <100 mg/dl for diabetics with no coronary vascular disease (CVD) and a level <70 mg/dl for those with CVD. Statins are the recommended treatment for lowering LDL. The purpose of this study is to assess the compliance of physicians at the University of Oklahoma College of Medicine, Tulsa, Family Medicine Clinic (OU-FMC) in following the recommendations by the Standards of Medical Care in Diabetes for blood pressure and LDL in type 2 diabetes mellitus (DM2). METHODS This is a retrospective study to evaluate treatment of LDL and high blood pressure in patients with DM2 as set forth by ADA recommendations. A sample of 200 patients both male and female (ages 18-100) with the diagnosis of DM2 from the OU-FMC electronic medical records (EMR) were evaluated for provider adherence to the ADA recommendations. Compliance was determined by those given an ACEI/ARB for outside goal blood pressure, and a statin for those with elevated LDL. RESULTS Of the 183 patients included in this study, 73 (50.3%) received a diagnosis of hypertension (HTN), 18 (9.8%) received a diagnosis of hyperlipidemia (HL) and 92 (39.9%) had both diagnoses. Of those diagnosed with HTN (165), 158 (95.8%) were in compliance. The most common ARB/ACEI was lisinopril (56.8%). Patients that received a diagnoses of HL (110), 86 (78.2%) were in compliance with the recommendations. The most prescribed statin was atorvastatin (55.2%). Demographically, the population was divided into 37% males and 63% females. The predominating payer source was Medicaid and Medicare (68.3%) and the remaining were combined self and private payers. CONCLUSION The results show that the University of Oklahoma Department of Family Medicine has been adhering to the guidelines recommended per the Standards of Medical Care for Diabetes by the ADA. Statins and ACEI/ARB were prescribed to patients based on these recommendations in the OU Family Medicine Clinic.