Download
1 / 40
400 likes | 547 Views
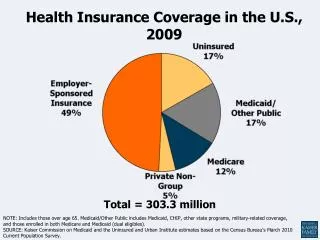
Health Insurance Coverage and Access in Rural America. Timothy D. McBride, PhD September 20, 2004. The Uninsured in the United States. Type of Health Insurance Coverage for the U.S. Non-Elderly Population, 2003. 45.0 million people without health insurance.

E N D
Health Insurance Coverage and Access in Rural America Timothy D. McBride, PhD September 20, 2004
Type of Health Insurance Coverage for the U.S. Non-Elderly Population, 2003 45.0 million people without health insurance Source: U.S. Census Bureau (2004).
Rise in the Uninsured Millions of Persons and Percentage of Population, 1987-2002 Number uninsured, and uninsurance rate, constantly rising Source: U.S. Bureau of the Census (2004), based on Current Population Survey (CPS). Note: CPS questions redesigned in 1999, 1997, and in the 1992-94 period.
Health Insurance Coverage in Rural America Results by: Erika Ziller, Andy Coburn, Cathy Hoffman, Sharon Loux, Timothy McBride Kaiser Family Foundation (2003) Data Source: Medical Expenditure Panel Survey (MEPS), 1996-1998
Urban-Rural County ComparisonNonelderly, 1998 Urban Counties 192 million Rural - Adjacent to Urban Counties 22 million Rural – Not Adjacent to Urban Counties (Remote) 22 million
Sources of Health Insurance Coverage(Age 0 – 64, December 1998) Rural Non Adjacent (RNA) residents are far less likely to have private coverage, and more likely to have Medicaid or other public coverage. Nearly one-fourth are uninsured.
Trend: Percent of Nonelderly Uninsured, December 1996-1998 The uninsured rate for those living in RNA remained unchanged from 1996 to 1998 in contrast to declines for urban and RA residents.
Trend: Percent of Nonelderly Uninsured All Year, December 1996-1998 RNA residents were one-third more likely to be uninsured all of 1998. From 1996-98, RA and Urban rates decreased or stayed the same while the rate for RNA residents increased.
Figure 14 200% or more of FPL* 100-199% FPL* <100% FPL*
Key Employment Factors Driving Health Insurance Gaps in Rural Counties • Size of Rural Businesses • Wage-Scale of Rural Workers
A Profile of the Rural and Urban Uninsured • Among the uninsured in rural non-adjacent counties: • 68% come from families where there is at least one full-time worker; • almost two-thirds come from low-income families (less than 200% of the federal poverty level) compared to half of the urban uninsured (almost half of the population in rural, non-adjacent counties are low-income families); • 30% are children;
A Profile of the Rural and Urban Uninsured • The rural uninsured are more likely to be white, non-Hispanics, in part reflecting the higher concentration of whites in rural America (83% vs. 67% in urban counties); • Self-reported health status is generally poorer than for the urban uninsured; and, • Families with two full-time workers and married couples are at higher risk of being uninsured if they live in a rural, non-adjacent area—where job-based health benefits are less available and incomes are lower.
Percent of Adults Uninsured, by Employment Status and Residence, 1998 There is no rural-urban difference in the uninsured rate for adults who are unemployed or OLF. The rate is higher for rural than urban workers.
Employer-Sponsored Health Insurance among Workers: Offer, Enrollment, and Coverage, 1998 The lower rate of ESI among RNA workers stems from lower employer offers; take up rates are the same for all three residence types.
Percent Uninsured among Self-Employed Workers by Residence, 1998 Self-employed rural workers living in rural counties are far more likely to be uninsured than those living in urban counties.
Key Characteristics of Uninsured Workers • Regardless of where a worker lives, working for a business with fewer than 20 employees more than doubles the risk of being uninsured • This is pronounced for RNA, where ⅓ of small business workers are uninsured compared to ¼ of urban workers with small employers. • Low-wage workers (< $7 per hour) are about 3 times more likely to be uninsured no matter where they live.
Firm Size among Uninsured Workers and Total Working Population by Residence, 1998 Rural Not Adjacent Rural Adjacent Urban RNA workers are the most likely to work for small business. More than 2/3 of uninsured RNA workers work for firms with < 20 employees.
Wages of Uninsured Workers and Total Working Population by Residence, 1998 Rural Not Adjacent Rural Adjacent Urban One-third of RNA workers earn less than $7 per hour. 60% of uninsured workers in RNA areas earn low wages compared to 40% in urban areas.
Dental and Prescription Drug Coverage among Privately Insured, MEPS, 2000 Rural residents with private health insurance are less likely to have dental or prescription drug coverage.
Privately Insured Individuals Who “Never” Go to the Dentist, MEPS, 2000 Rural residents are 50% more likely to report they never go to the dentist.
Mean Out-of-Pocket Expenditures among Privately Insured, MEPS, 2000 Rural residents with private coverage have higher OOP expenses, suggesting their benefits are less comprehensive than in urban areas.
Mean Out-of-Pocket Dental Expenditures among Privately Insured, MEPS, 2000 Rural residents have higher OOP expenses for dental care, reflecting lower rates of dental coverage and potentially poorer benefits.
Time Since Last Physical Exam (Adults 18-64), MEPS, 1998 Adults in RNA areas have routine physical exams with less frequency than those in other areas.
Time Since Last Cholesterol Test (Adults 18-64), MEPS, 1998 Almost half of adults did not have a cholesterol test in the past 5 years, compared to only one-third of urban adults.
Time Since Last Pap Smear (Females 18-64), MEPS, 1998 Women in RNA areas were 50% more likely to have gone without a pap smear in the last five years than urban women were.
Time Since Last Mammogram (Females 39-64), MEPS, 1998 More than one-third of RNA women aged 39-64 had not had a mammogram in the prior two years, compared to only one-fourth of urban women.
Not All Rural Places & People Are the Same • National surveys and reports overlook sometimes dramatic differences between rural, non-adjacent, other rural, and urban residents. • Policy-makers need to understand that not all rural areas are the same in order to design and implement effective reform strategies.
Differences in Characteristics Have Important Policy Implications • Strategies to increase health insurance among rural residents should have a long-term focus • Many of the rural uninsured, particularly those in counties not adjacent to an urban area, lack insurance for long periods of time. • These strategies would contrast with past federal reforms, such as COBRA or HIPAA, which provide transitional insurance coverage.
Rural Residents Depend on the Medicaid & SCHIP Program for Coverage • The Medicaid and SCHIP programs are a vital coverage option for many rural residents because: • They are less likely to be offered employer-based coverage, and • They have lower wages and incomes that allow them to qualify for Medicaid/SCHIP. • Any erosion in Medicaid/SCHIP eligibility or benefits would adversely affect rural areas
Rural Economic Realities Are Critical to Expanding Insurance Coverage • Efforts to increase enrollment in private health insurance, either through employer or individual plans, would require generous subsidies: • Financial fragility of small rural employers • Lower wages and incomes of rural workers