Download
1 / 72
820 likes | 2.15k Views
HYPERTENSION Up to date. K.Premmatat M.D. Overview. Epidermiology Pathophysiology Classification & Definition Secondary hypertension , white – coat hypertension , masked hypertension Role of HBPM Patient assessment & risk factors Treatments.

E N D
HYPERTENSIONUp to date K.Premmatat M.D.
Overview • Epidermiology • Pathophysiology • Classification & Definition • Secondary hypertension , white – coat hypertension , masked hypertension • Role of HBPM • Patient assessment & risk factors • Treatments
What is the estimated prevalence of hypertension in Thailand ?
Rule of halves • Only ½ have been diagnosed. • Only ½ of those diagnosed have been treated. • Only ½ of those treated are adequately controlled.
Pathophysiology Salt ,RAAS , Intravascular volumes Autonomic nervous system (NE,E,DA)
Complications • Atherosclerotic event • CAD (coronary artery disease) • CVA (Cerebral vascular accident) • PAD (Peripheral artery disease) • CKD (Chronic kidney disease) • Retina
Population Based Strategy for Hypertension Reduction. Graph depicts Systolic Blood pressure distributions in a population with a change in Blood pressure and the % reduction in mortality associated with this. JNC-7; 2003.
Classification & Definition • JNC 7 • 2013 ESH/ESC • NICE guidance UK • Essential (Primary) • Secondary • White – coat • Masked
NICE guidance UK • Stage 1 hypertension: • Clinic blood pressure (BP) is 140/90 mmHg or higher and • ABPM or HBPM average is 135/85 mmHg or higher. • Stage 2 hypertension: • Clinic BP 160/100 mmHg is or higher and • ABPM or HBPM daytime average is 150/95 mmHg or higher. • Severe hypertension: • Clinic BP is 180 mmHg or higher or • Clinic diastolic BP is 110 mmHg or higher.
Secondary hypertension • Renal • Parenchymal disease (DN , AGN , CGN) • Renal cysts (Polycystic kidney disease) • Renal tumor(including rennin - secreting tumor) • Obstructive uropathy • Primary sodium retention (Liddle syndrome) • Renal artery stenosis • Arteriosclerotic • Fibromuscular dysplasia
Secondary hypertension • Adrenal • Primary aldosteronism • Cushing syndrome • Pheochromocytoma • Congenital adrenal hyperplasia • Licorice • Aortic coarctation • Obstructive sleep apnea • Preeclampsia / eclampsia
Secondary hypertension • Neurogenic • Polyneuritis (Acute porphyria , lead poisoning) • Acute increased ICP • Acute spinal cord dissection • Endocrine • Hyper/ hypothyroidism • Hypercalcemia (Hyperparathyroidism) • Acromegaly , carcinoids • Medications steriod , estrogen (high dose) , TCAs , decongestant , NSAIDs , MAOI , nicotine , cocaines , EPOs
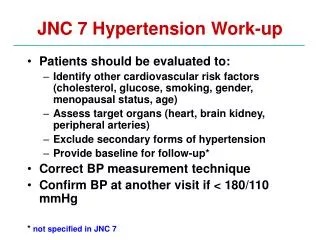
When we should think for secondary hypertension ? • History & physical examinations • Hypertension in the young • Refractory hypertension • Uncontrolled hypertension • First diagnosis hypertension in patient > 55 year old
White – coat hypertension Masked hypertension • White – coat hypertension • Grade I hypertension in the office but normal at home. • High office BP in individuals without asymptomatic organ damage and at low total CV risk. • Masked hypertension • High normal BP in the office but hypertension at home. • Normal office BP in individuals with asymptomatic organ damage or at high total CV risk.
HMBP (Home blood pressure monitoring) • Indication • Suspicious white – coat , masked hypertension • Considerable variability of office BP over the same or different visits • Autonomic, postural, post-prandial, siesta- and drug-induced hypotension • Elevated office BP or suspected pre-eclampsia in pregnant women • Identification of true and false resistant hypertension
Patient assessment & risk factorsTreatments • Level of BP • Risk factors • Target organ damaged
Treatments • Goal of treatments • Line of management • - Life – style modification • - Drug • - Compelling indication • - Special conditions • Follow up
Goal of treatments • JNC 7 • Treat to BP <140/90 mmHg or BP <130/80 mmHg in patients with diabetes or chronic kidney disease. • NICE • 140/90 mmHg in people aged under 80 • 150/90 mmHg in people aged 80 and over • 130/80 mmHg in people who have diabetes , CKD • 125/75 mmHg in people who have proteinuria >= 1 g/day
Goal of treatments • ESC 2013 • All 140/90 mmHg • Except • DM 140/85 mmHg • Elderly > 80 year olds DM 140-150/90 mmHg NON - DM 140-150/85 mmHg
Line of management LSM – Life - style modifications • JNC , NICE , ESC SAME
Life - style modifications • DASH (Dietary approachs to stop hypertension) • Aerobic exercise • Avoid tobacco , Alcohol drinking (male < 2 drink/day = beer 720 ml , female < 1drink/day ) • Restrict salt • Weight reduction
Drugs • Diuretic • Beta – blocker • ACEI • ARB • CCB • Alpha – blocker • Aldosterone – antagonists eg. Spironolactone , eplerenone • Direct vasodilatoreg. Hydralazine , minoxidill • Sympatholytic drug eg. clonodine
Without Compelling Indications With Compelling Indications Drug(s) for the compelling indications Other antihypertensive drugs (diuretics, ACEI, ARB, BB, CCB) as needed. Stage 1 Hypertension(SBP 140–159 or DBP 90–99 mmHg) Thiazide-type diuretics for most. May consider ACEI, ARB, BB, CCB, or combination. Stage 2 Hypertension(SBP >160 or DBP >100 mmHg) 2-drug combination for most (usually thiazide-type diuretic and ACEI, or ARB, or BB, or CCB) Not at Goal Blood Pressure Optimize dosages or add additional drugs until goal blood pressure is achieved.Consider consultation with hypertension specialist. Algorithm for Treatment of Hypertension JNC7 Lifestyle Modifications Not at Goal Blood Pressure (<140/90 mmHg) (<130/80 mmHg for those with diabetes or chronic kidney disease) Initial Drug Choices
Aged over 55 years or black person of African or Caribbean family origin of any age Summary of antihypertensive drug treatment (NICE) Aged under55 years Step 1 C A Key A – ACE inhibitor or low-cost angiotensin II receptor blocker (ARB) C – Calcium-channel blocker (CCB) D – Thiazide-like diuretic Step 2 A + C Step 3 A + C + D Resistant hypertension A + C + D + consider further diureticor alpha- or beta-blocker Consider seeking expert advice Step 4