Download
1 / 24
250 likes | 391 Views
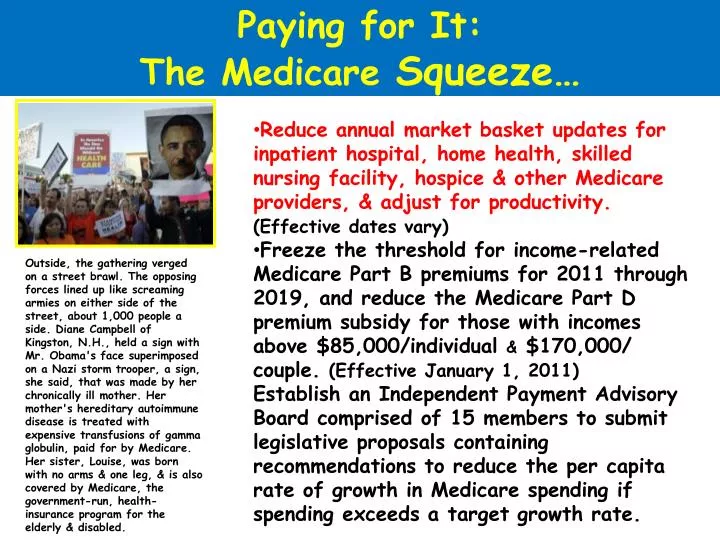
Paying for It: The Medicare Squeeze…. Reduce annual market basket updates for inpatient hospital, home health, skilled nursing facility, hospice & other Medicare providers, & adjust for productivity. (Effective dates vary)

E N D
Paying for It: The Medicare Squeeze… • Reduce annual market basket updates for inpatient hospital, home health, skilled nursing facility, hospice & other Medicare providers, & adjust for productivity. (Effective dates vary) • Freeze the threshold for income-related Medicare Part B premiums for 2011 through 2019, and reduce the Medicare Part D premium subsidy for those with incomes above $85,000/individual & $170,000/ couple. (Effective January 1, 2011) • Establish an Independent Payment Advisory Board comprised of 15 members to submit legislative proposals containing recommendations to reduce the per capita rate of growth in Medicare spending if spending exceeds a target growth rate. Outside, the gathering verged on a street brawl. The opposing forces lined up like screaming armies on either side of the street, about 1,000 people a side. Diane Campbell of Kingston, N.H., held a sign with Mr. Obama's face superimposed on a Nazi storm trooper, a sign, she said, that was made by her chronically ill mother. Her mother's hereditary autoimmune disease is treated with expensive transfusions of gamma globulin, paid for by Medicare. Her sister, Louise, was born with no arms & one leg, & is also covered by Medicare, the government-run, health-insurance program for the elderly & disabled.
Paying for It: The Medicare Squeeze… • Reduce Medicare Disproportionate Share Hospital (DSH) payments initially by 75% and subsequently increase payments based on the percent of the population uninsured and the amount of uncompensated care provided.(Effective FY 2015) • Eliminate the Medicare Improvement Fund. (Effective upon enactment) • Allow providers organized as accountable care organizations (ACOs) that voluntarily meet quality thresholds to share in the cost savings they achieve for the Medicare program. To qualify as an ACO, organizations must agree to be accountable for the overall care of their Medicare beneficiaries, have adequate participation of primary care physicians, • Define processes to promote evidence-based medicine, report on quality and costs, and coordinate care. (Shared savings program established 1/1/2012)
Paying for It: The Medicare Squeeze… • Create an Innovation Center within the Centers for Medicare & Medicaid Services to test, evaluate, and expand in Medicare, Medicaid, and CHIP different payment structures and methodologies to reduce program expenditures while maintaining or improving quality of care. Payment reform models that improve quality and reduce the rate of cost growth could be expanded throughout the Medicare, Medicaid, and CHIP programs. (Effective 1/1/2011) • Reduce Medicare payments that would otherwise be made to hospitals by specified percentages to account for excess (preventable) hospital readmissions. (Effective 10/1/2012) • Reduce Medicare payments to certain hospitals for hospital-acquired conditions by 1% (Effective FY 2015)
COSTS & COVERAGE MEDICARE SAVINGS: Squeeze roughly $500 billion out of the projected growth in Medicare over 10 years, including $178 billion in cuts to federal subsidies for privately offered Medicare Advantage plans, which now cost the government 14% more on average than traditional Medicare • FLEXIBLE SPENDING ACCOUNTS: Starting in 2013, would place a $2,500 annual limit on what people can set aside from their paychecks before paying taxes to use for health care expenses. • TANNING TAX: Would impose a 10% tax on indoor tanning services starting in 2010.
Paying for It: Squeezing Medicaid Too… • Increase the Medicaid drug rebate percentage for brand name drugs to 23.1 (except the rebate for clotting factors & drugs approved exclusively for pediatric use increases to 17.1%); • Increase the Medicaid rebate for noninnovator, multiple source drugs to 13% of average manufacturer price; • Extend the drug rebate to Medicaid managed care plans. (Effective 1/1/2010) • Reduce a state’s Medicaid DSH allotment by 50% or 25% for low DSH states (and by lesser percentages for states meeting certain criteria) once the state’s uninsured rate decreases by at least 45%. DSH allotments will be further reduced, not to fall below 50% of the total allotment in 2012 if states’ uninsured rates continue to decrease. Exempt any portion of the DSH allotment used to expand Medicaid eligibility through a section 1115 waiver. (Effective 10/1/2011) • Prohibit federal payments to states for Medicaid services related to health care acquired conditions. (Effective 7/1/2011)
Gosh dern those GuvmintBurracrats! NOW THEY WANT TO PAY ONLY FOR “QUALITY CARE” (and only THEY can define “quality”) On May 16, 2011, it was announced that future payment increases to hospitals will depend upon each hospital meeting exacting new “quality indicators” and that hospitals failing to meet these quality standards will not get their payments increased. HOW DARE THEY! GOVERNMENT BUREAUCRATS RUNNING HEALTH CARE! It’s what Palin, Beck, Hannity & O’Reilly have been warning us about! SOCIALIZED MEDICINE! Government bureaucrats telling us how to run health care. John Boehner was reduced to tears upon hearing the news!
Gosh dern those GuvmintBurracrats! Oops, not so fast. It wasn’t the government that announced this new change, it was Wellpoint/Anthem (the nation’s largest for-profit private health insurer). Starting July 1, 2011 hospitals serving Wellpoint/Anthem insureds must report on 51 so-called “quality indicators,” … measuring outcomes (55%), patient-safety (35%) & patient-satisfaction (10%).
$230B CBO vs. Actuary vs. Do Nothing $150B $100B $50B -0- -$50 -$100B -$200B -$400B $143B CBO Actuary -$96B Do Nothing -$320B 2010 2012 2104 2016 2018 2020
Obama: The H&%# With the SGR… at Least as Far as The Docs are Concerned Beginning April 2013, require the Medicare Chief Actuary to project whether Medicare per capita spending exceeds the average of CPI-U & CPI-M, based on a five year period ending that year. If so, beginning January 15, 2014, the Board will submit recommendations to achieve reductions in Medicare spending. Beginning January 2018, the target is modified such that the board submits recommendations if Medicare per capita spending exceeds GDP per capita plus one percent. The Board will submit proposals to the President & Congress for immediate consideration. The Board is prohibited from submitting proposals that would ration care, increase revenues or change benefits, eligibility or Medicare beneficiary cost sharing (including Parts A & B premiums), or would result in a change in the beneficiary premium percentage or low-income subsidies under Part D. Hospitals & hospices (through 2019) & clinical labs (for one year) will not be subject to cost reductions proposed by the Board. The Board must also submit recommendations every other year to slow the growth in national health expenditures while preserving quality of care by January 1, 2015.
IMPLEMENTATION TIMELINE Most of the New Law Will Take Years to Implement Implement PPACA & call me again in 2014
Health Rationing … er, I mean “Comparative Effectiveness”
Let’s Kill Granny! Health Care Rationing Trust me on this, I’m a lawyer… just like his Democratic predecessor in the presidency, Bill Clinton, who was somewhat successful at reaching across the aisle, Barack Obama has not hesitated to “steal” a good Republican ideal & turn it to good (political) use. Republicans (without a single Democratic vote) passed the “Medicare Modernization Act of 2003.” Buried in that 717-page law were provisions for CMS to begin the process of determining the “comparative effectiveness” of various health care services. The current health care plans simply build on that initial step… but oops, that’s where “killing granny” became an issue. KILL GRANNY!
“Outcomes Research” and (gasp) Health Care “Rationing” The GOP-passed 2003 Medicare Modernization Act (better known for establishing the Part D drug program) had lots of buried secrets, not the least of which was new funding for AHRQ and a plan to begin several demonstration projects with a goal of better identifying… • “the appropriate use of best practice guidelines by providers and services by beneficiaries” • The “reduced scientific uncertainty” in the delivery of care through the examination of variations in the utilization and *allocation of services, and outcomes measurement and research” • achieving the “*efficient allocation of resources” • “the financial effects on the health care marketplace of altering the incentives for care delivery and changing the *allocation of resources” HIPAA facilitates the collection of data and thus the ability of planners and payers to ration health care intelligently. (* Trust me on this, I’m a lawyer, “allocation of resources” = “rationing”) theJeanneScottletter
Future of US Health Care: “Rationing” … by any other name Election 2008: the Winners & Losers The little agency that could. Buried in the backwater reaches of the U.S. Public Health Service is the Agency for Healthcare Research & Quality (AHRQ), charged with developing the future “cookbook of health care.” CM2 has already embarked on an effort to define many of the elements of effective health care, that is what works and what doesn’t, using much of the work product of AHRQ. “In the future, we will only pay for what works and not for what doesn’t work.” President George W. Bush, September 17, 2006
But Fox News says Bush’s plan, er, I mean “Obama’s plan” is really “Rationing”
Worthless Lives Under the British NHS “People such as scientist Stephen Hawking wouldn't have a chance in the U.K., where the National Health Service would say the life of this brilliant man, because of his physical handicaps, is essentially worthless.” Investors Business Daily, August 11, 2009 Apparently, Investor’s Business Daily doesn’t have access to the Internets. A quick stop at Wikipedia would have told them that Hawking is British, lives in Britain, and has lived to the age of 67 there, and was diagnosed with ALS under, and treated by the National Health Service for his entire adult life. They must have just been fooled by his voice synthesizer's American accent. "I wouldn't be here today if it were not for the NHS. I have received a large amount of high-quality treatment without which I would not have survived." Stephen Hawking, at a press conference after being awarded the USA’s highest civilian award, the Presidential medal of Freedom, August 12, 2009.
How Efficient Allocation of Resources (i.e., “Rationing”) Would Work Collect all-population, all-patient, all-payer data (including care processes, clinical outcomes, patient experiences, and costs while enabling benchmarking and monitoring of changes) Assess health outcomes (e.g., percent diabetes under control; cancer survival rates) Post web comparison of insurance choices, costs and benefits, experiences; include share of premium for administrative/overhead/profit (complete national transparency with capacity for state or geographic analysis and benchmarks and designed so states could add, build with more detailed data where available) And someday… start paying only for what works and not for what doesn’t
IS “COMPARATIVE EFFECTIVENESS” SIMPLY ANOTHER WAY OF SAYING “RATIONING?” In the U.K., the National Heath Service (the nationalized health program) has instituted a National Institute for Health & Clinical Excellence (NICE). NICE has used cost calculations per "quality adjusted life-year (QALY)" saved as an index for what NHS will or will not cover. Anything that costs more than £30,000 British pounds (about $54,000 U.S.) per QALY saved can only be covered after undergoing a further extensive cost-benefit analysis.
IS IT MEASURING THE VALUE OF HUMAN LIFE? The quality-adjusted life year (QALY) is a measure of disease burden, including both the quality and the quantity of life lived. It is used in assessing the value for money in a medical intervention. The QALY is based on the number of years of life that would be added by the intervention. Each year in perfect health is assigned the value of 1.0 down to a value of 0.0 for death. If the extra years would not be lived in full health, e,g., if the patient would lose a limb, or be blind or have to use a wheelchair, then the extra life-years are given a value between 0 and 1.