Download

1 / 16
160 likes | 233 Views
Early Results of Costs and Utilization, Virginia Coordinated Care Delivery System. Wally R. Smith, MD, Donna K. McClish , PhD, Patricia Carcaise-Edinboro , PhD, Gloria Bazzoli , PhD, Alton Hart, MD, MPH, Arline Bohannon, MD, Peter Boling, MD, Sheldon Retchin , MD, MPH, MSHA

E N D
Early Results of Costs and Utilization, Virginia Coordinated Care Delivery System Wally R. Smith, MD, Donna K. McClish, PhD, Patricia Carcaise-Edinboro, PhD, Gloria Bazzoli, PhD,Alton Hart, MD, MPH, Arline Bohannon, MD,Peter Boling, MD,Sheldon Retchin, MD, MPH, MSHA Virginia Commonwealth University AHRQ MD-10-012
Background • Uninsured • Utilization patterns similar to Medicaid, underinsured • Poor • Lower social support • Less transportation, education, delayed gratification • May use ED rather than PCP • Health Care Reform • Reduces the number of uninsured, underinsured • Of the 46 million uninsured, estimated 32 million will soon be covered • Expands Medicaid program to approximately 16 million newly insured
Do the Newly Insured Poor Change Utilization Patterns? • Not in some studies of providing managed care insurance-like programs to uninsured • Barriers and Weaknesses of previous programs • Short duration • Dose of managed care variable • Little case management • Poor PCP (geographic or time) availability • Few barriers to ED access • Comorbidity mix unfavorable
Virginia Coordinated Care 2000-present • Patient-Centered Medical Home Insurance-like program for uninsured • Uses managed care principles • All patients qualify for the Indigent care program supported by federal DSH and State General funds • Primary care provided by community PCP’s funded by VCUHS profits from commercial plans • FFS and Management fee paid to PCPs in urban communities surrounding VCU • Catchment area within 30 miles of VCU • Patients given card with PCP’s name • Case managers support, assist with ∆’s, • Enrollment files managed by Medicaid HMO owned by VCU Health System
Initial Evaluation of VCC • Lower ED visit rates • Patients saw PCP • VCC off-loaded patients to community physicians • Community physicians happy with management fees • Case management dose small • Short-term evaluation only
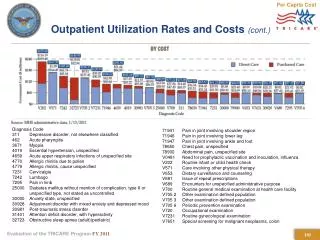
How Did VCC Enrollment, Costs, and Utilization Grow from 2003-2005? Utilization? Per Member Per Month (PMPM) Costs? Uptake by community PCP’s? Relative costs?
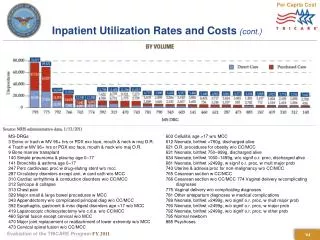
PMPM Costs by Svc Type * Missing ED data for Richmond Community Hospital FY03, all data for FY05 incomplete
Conclusions-1 There was a 12% annual increase, and a 25% increase overall, in VCC enrollment from FY 2003-2005. Simultaneously, community practitioner member months increased 28%. Per member per month costs rose slightly for pharmacy and ED, but were flat for inpatient and outpatient services.
Conclusions-2 Overall, the percentages of VCC pts seeking primary care slightly increased, but so did the percentage w all other visits. Specialty care utilization percentages dropped slightly. Uptake %’s by community primary care mirrored dropoff %’s by VCU primary care. Community primary care PMPM rose, but was more than offset by decreases in university primary care PMPM, leading to a decrease in PMPM for these segments combined. Specialty care PMPM remained flat.
ED PMPM Details * Missing ED data for Richmond Community Hospital FY03, all data for FY05 incomplete