Download
1 / 47
510 likes | 989 Views
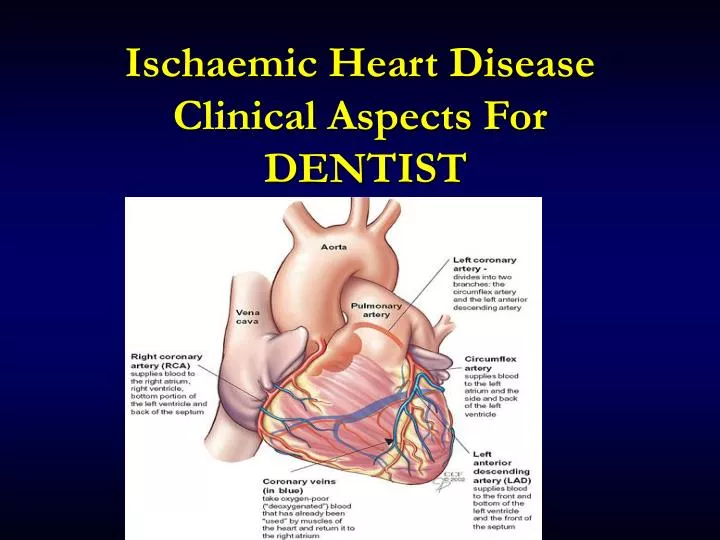
Ischaemic Heart Disease Clinical Aspects For DENTIST. Coronary Heart Disease. A leading cause of SICKNESS and DEATH. Risk Factors for Cardiovascular Disease. Hypertension High cholesterol Obesity Cigarette smoking Physical inactivity Diabetes mellitus Kidney disease

E N D
Coronary Heart Disease A leading cause of SICKNESS and DEATH
Risk Factors for Cardiovascular Disease • Hypertension • High cholesterol • Obesity • Cigarette smoking • Physical inactivity • Diabetes mellitus • Kidney disease • Older age (>55 ♂; > 65 ♀) • Family history of premature cardiovascular disease • Obstructive sleep apnea • Periodontal disease ?
Coronary Heart Disease: Myocardial Ischemia • Decreased blood supply (and thus oxygen) to the myocardium that can result in acute coronary syndromes: • Angina pectoris ( Stable ) • Unstable Angina • Myocardial infarction • Sudden death (due to fatal arrhythmias)
Ischaemic heart diseaseDefinition • An imbalance between the supplyofoxygen and the myocardialdemand resulting in myocardial ischaemia. • Anginapectoris symptom not a disease chest discomfort associated with abnormal myocardial function in the absence of myocardial necrosis • Supply • Atheroma, thrombosis, spasm, embolus • Demand • Anaemia, hypertension, high cardiac output (thyrotoxicosis, myocardial hypertrophy)
Ischaemic heart diseaseManifestations • Sudden death • Acute coronary syndrome ( Myocardial Infarction & Unstable Angina ) • Stable angina pectoris • Heart failure • Arrhythmia • Asymptomatic
Ischaemic heart diseaseEpidemiology • Commonest cause of death in the Western world. (up to 35% of total mortality) • Over 20% males under 60 years have IHD • Health Survey : 3% of adults suffer from angina 1% have had a myocardial infarction in the past 12 months
Ischaemic heart diseaseAetiology • Fixed • Age, Male, +ve family history • Modifiable – strong association • Dyslipidaemia, smoking, diabetes mellitus, obesity, hypertension • Modifiable - weak association • Lack of exercise, high alcohol consumption, type A personality, OCP, soft water Atherosclerosis
Risk Factors for Ischemic Heart Disease • Family History • Smoking • Hypertension • Diabetes Mellitus • Hypercholesterolaemia • Lack of exercise Obesity • Age & Sex • PRIMARY PREVENTION
Spectrum of the Atherosclerotic Process • Coronary Arteries (angina, MI, sudden death) • Cerebral Arteries (stroke) • Peripheral Arteries (claudication)
Ischaemic heart diseaseAcute coronary syndromes Atherosclerosis Coronary Artery spasm Fatal / Non-Fatal AMI Unstable Angina
Warning Signs and Symptoms of Heart attack • Pressure, fullness or a squeezing pain in the center of your chest that lasts for more than a few minutes. • Pain extending beyond your chest to your shoulder, arm, back or even your teeth and jaw. • Increasing episodes of chest pain • Prolonged pain in the upper abdomen • Shortness of breath- may occur with or without chest discomfort • Sweating • Impending sense of doom • Lightheadedness • Fainting • Nausea and vomiting
Angina Pectoris • At least 70% occlusion of coronary artery resulting in pain. What kind of pain? • Chest pain • Radiating pain to: • Left shoulder • Jaw • Left or Right arm • Usually brought on by physical exertion as the heart is trying to pump blood to the muscles, it requires more blood that is not available due to the blockage of the coronary artery(ies) • Is self limiting usually stops when exertion is ceased
Clinical Patterns of Angina Pectoris • Stable - pain pattern and characteristics relatively unchanged over past several months (better prognosis) • Unstable - pain pattern changing in occurrence, frequency, intensity, or duration (poorer prognosis); MI pending
TREATMENT MEDICATIONS • Nitrates- vasodilator eg: ISDN. ISMN • Pain reliever- eg: Morphine • Beta-blockers • Statins- cholesterol lowering drugs. Eg: Atorvastatin, Simvastatin
Ischaemic heart diseaseRelevance to Dentistry • IHD is common • Subjects with IHD have more severe dental caries and periodontal disease – association or causation? • Angina is a cause of pain in the mandible, teeth or other oral tissues • Stress provokes ACS!
Myocardial Infarction • Partial or total occlusion of one or more of the coronary arteries due to an atheroma, thrombus or emboli resulting in cell death (infarction) of the heart muscle • When an MI occurs, there is usually involvement of 3 or 4 occluded coronary vessels
Chest PainMyocardial ischaemia • Site Jaw to navel, retrosternal, left submammary • Radiation Left chest, left arm, jaw….mandible, teeth, palate • Quality/severity tightness, heaviness, compression…clenched fists • Precipitating/relieving factors physical exertion, cold windy weather, emotion rest, sublingual nitrates • Autonomic symptoms sweating, pallor, peripheral vasoconstriction, nausea and vomiting
Chest PainDifferential diagnosis • Cardiacpathology • Pericarditis, aortic dissection • Pulmonarypathology • Pulmonary embolus, pneumothorax, pneumonia • Gastrointestinalpathology • Peptic ulcer disease, reflux, pancreatitis, ‘café coronary’ • Musculoskeletalpathology • Trauma, Tietze’s Syndrome
Acute Myocardial InfarctionAssessment • 30% of deaths occur in the first 2 hours. (Cardiac muscle death occurs after 45 mins of ischaemia) • Symptoms and signs of myocardial ischaemia • Also • Changes in heart rate /rhythm • Changes in blood pressure
Acute Myocardial InfarctionConfirming the diagnosis • Typical chest pain • Electrocardiographic changes • ST elevation • new LBBB • Myocardial enzyme elevation • Creatine kinase (CK-MB) • Troponin
Acute Myocardial InfarctionTreatment • Stop dental treatment • Call for help • Rest, sit up and reassure patient • Oxygen • Analgesia (opiate, sublingual nitrate) • Aspirin • Thrombolysis • Primary angioplasty • Beta-Blockers • ACE inhibitors • Prepare for basic life support
Surgical Treatment • Percutaneous Transluminal Coronary Angioplasty (PTCA) • balloon expansion that can provide 90% dilitation of vessel lumen
Stent Placement • With use of just the balloon, re-occlusion of the artery can occur within months • Placement of a stent delays or prevents re-occlussion
Surgical Treatment • Coronary Artery By-Pass Graft (CABG) • The graft bypasses the obstruction in the coronary artery • Graft sources: • saphenous vein • internal mammary artery • radial artery
Acute Myocardial InfarctionComplications • Sudden Death (18% within 1 hour,36% within 24 hours) • Non-fatal arrhythmia • Acute left ventricular failure • Cardiogenic shock • Papillary muscle rupture and mitral regurgitation • Myocardial rupture and tamponade • Ventricular aneurysm and thrombus • Distal Embolisation
Sudden Death • Sudden Cardiac Death is also known as a “Massive Heart Attack” in which the heart converts from sinus rhythm to ventricular fibrillation • In V-Fib, the heart is unable to contract fully resulting in lack of blood being pumped to the vital organs • V-Fib requires shock from defibrillator “SHOCKABLE RHYTHM”
Dental Considerations • Assessment and Overall Management • Pharmaceuticals • Emergency Situations • Oral Effects of Pharmaceuticals • Antibiotic Prophylaxis • Post MI: when to treat • Consider three areas: • How severe or stable the ischemic heart disease is • The emotional state of the patient • The type of dental procedure
RISK • Major Risk for Perioperative Procedures: • Unstable Angina (getting worse) • Recent MI • Intermediate Risk for Perioperative Procedures: • Stable Angina • History of MI • Most dental procedures, even surgical procedures fall within the risk of less than 1% • Some procedures fall within an intermediate risk of less than 5% • Highest risk procedures those done under general anesthesia
Management for Low-Intermediate Risk • Short appointments • AM appointments • Comfort • Vital Signs Taken • Avoidance of Epinephrine within Local Anesthetic or Retraction Cord • O2 Availability
Dentistry & Cardiovascular Medicine • AMI • GA within 3/12 of AMI: 30% re-infarction rate @ 1/52 post op • Avoid routine LA dental treatment for 3/12 (emergency treatment only) • Avoid excess dosage, reduce anxiety • Avoid elective surgery under GA for1 year (specialist) • Be aware of medications (bleeding, hypotension)
Post MI: When to Treat • Why delay treatment? • Remember that with an MI there is damage to the heart, be it severe or minimal that may effect the patient’s daily life • MI within 1 month Major Cardiac Risk • MI within longer then 1 month: • Stable routine dental care ok • Unstable treat as Major Cardiac Risk • Older studies suggest high re-infarction rates when surgery performed within 3 months, 3-6 months… however, this was abdominal and thoracic surgery under general anesthesia • New research suggests delaying elective tx for 1 month is advisable. Emergent care should be done with local anesthetic without epinephrine and monitoring of vital signs • When in doubt: • CONSULT THE CARDIOLOGIST
Dental Management Correlate • Elective dental care is ok if it has been longer than 4-6 weeks since the MI and the patient does not report any ischemic symptoms. • If there is any doubt or question, consult with the cardiologist.
Dental Considerations for IHD • Common Situations: • Orthostatic Hypotension due to use of anti-hypertensives (beta blockers, nitroglycerin…) • Raise chair slowly • Allow patient to take his/her time • Assist patient in standing • Post-Op Bleeding: • When patients on Plavix or Aspirin, expect increased bleeding because of decreased platelet aggregation
Dental Considerations for IHD • Emergent Situations: • Possible MI: • Remember that pain in the jaw may be referred pain from the myocardium assess the situation, have good patient history, follow ABC’s • Angina: • In situations of angina pectoris, all operatories should have nitroglycerin to be placed sublingually
Dental Considerations for IHD • Emergent Situations: • Chest Pain-MI: • STOP PROCEDURE • Remove everything from patient’s mouth • Give sublingual nitroglycerin • Wait 5 minutes if pain persists, give more nitroglycerin, assume MI • 101 • Give chewable aspirin ABC’s
Dental Management: Stable Angina/Post-MI >4-6 weeks • Minimize time in waiting room • Short, morning appointments • Preop, intra-op, and post-op vital signs • Pre-medication as needed • anxiolytic (triazolam; oxazepam); night before and 1 hour before • Have nitroglycerin available – may consider using prophylacticaly • Use pulse oximeter to assure good breathing and oxygenation • Oxygen intraoperatively (if needed) • Excellent local anesthesia - use epinephrine, if needed, in limited amount (max 0.04mg) or levonordefrin (max. 0.20mg) • Avoid epinephrine in retraction cord
Dental Management:Unstable Angina or MI < 3 months • Avoid elective care • For urgent care: be as conservative as possible; do only what must be done (e.g. infection control, pain management) • Consultation with physician to help manage • Consider treating in outpatient hospital facility or refer to hospital dentistry • ECG, pulse oximetry, IV line • Use vasoconstrictors cautiously if needed
Intraoperative Chest Pain • Stop procedure • Give nitroglycerin • If after 5 minutes pain still present, give another nitroglycerin • If after 5 more minutes pain still present, give another nitroglycerin • If pain persists, assume MI in progress and activate the EMS • Give aspirin tablet to chew and swallow • Monitor vital signs, administer oxygen, and be prepared toprovide life support
Conclusion: • When treating patients with Ischemic Heart Disease or recent MI… • Use caution and common sense • When in doubt: • CONSULT THE CARDIOLOGIST