Download
1 / 35
350 likes | 351 Views
This article provides a critical review of Irritable Bowel Syndrome (IBS), discussing its epidemiology, etiology, pathogenesis, clinical presentation, diagnosis, treatment, and future needs. It also explores the role of FODMAPs in managing IBS symptoms and the development of post-infectious IBS.

E N D
Irritable Bowel SyndromeA functional or an organic condition?Ferrara, September 27th, 2014 Reinhold W. Stockbrugger Em. Prof. Gastroenterology and Hepatology, University Maastricht/NL Contract Prof. Internal Medicine, University Ferrara/I Editor European Journal of Gastroenterology & Hepatology rstockbrugger635@gmail.com
What is a functional condition? ? I do not function ? ? It functions me ? ? Am I healthy ? ? Sick leave for functional disorders ? ? Do I need a psychologist ? ? Or a pension ? ? Why has the doctor said that that (s)he cannot help me? I think (s)he does not function !!!
RS: body + soul?Fortunately much more! My parents (or the lack of them) The alcohol The politics The bugs My boss The weather The fast and slow food The sex The money The music The diabetes The sports The future and the anxiety
IBS – Critical Review 2014 epidemiology etiology, pathogenesis clinical presentation and diagnosis treatment outcome future needs
IBS – EpidemiologyIn Northern Greece Katsinelos et al. Eur J GastroenterolHepatol 2009; 21: 183-9 Setting: Primary Care, 2004 - 2007 N= 2397 (f: 70.6%; mean age 46.1 years) IBS in 15.7% (D-IBS 36.5%; C-IBS 44.2%; M-IBS 19.3%) IBS patients more likely to be: female from urban areas
IBS – EpidemiologyIn Asia Gwee et al. J GastroenterolHepatol 2009; 24: 1601-7 Early studies: prevalence <5% Now: Singapore 8.6% Tokyo 9.8% India: 4.2% Symptomatology different from Rome criteria
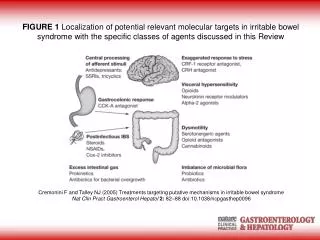
IBSEtiology, pathogenesis “The times, they are changing …” 1980 Motility 1990 Psychology 2000 Microbiology • Neurophysiology 2009 Motility, Metabolism, Diet 2014 FODMAPs (Fermentable Oligosaccharides Disaccharides Monosaccharaides And Polyols)
The Newcomer: FODMAPs “A diet low in FODMAPs reduces symptoms of Irritable Bowel Syndrome” Halmos E.P. et al. Gastroenterology 2014; 146: 67 – 75 • High FODMAP food (things to avoid / reduce) • Vegetables and Legumes • Garlic – avoid entirely if possible • Onions – avoid entirely if possible • Artichoke • Asparagus • Baked beans • Beetroot • Black eyed peas For this you really could need a dietician! • Broad beans • Butter beans • Cauliflower • Celery – greater than 5cm of stalk • Kidney beans • Leeks • Mange Tout • Mushrooms • Peas • Fruit – fruits can contain high fructose + other 121 items! • Apples • Apricots • Avocado • Blackberries • Cherries • Currants • Dates • Grapefruit • Lychee • Mango • Nectarines • Peaches • Pears • Persimmon • Plums • Prunes • Raisins • Tinned fruit in apple / pear juice • Watermelon • Cereals, Grains, Breads, Biscuits, Pasta, Nuts and Cakes • Wheat containing products such (be sure to check labels): • Biscuits • Breadcrumbs • Cashews • Cakes • Egg noodles • Regular noodles • Pastries • Pasta made from wheat • Udon noodles • Wheat bread • Wheat cereals • Wheat rolls • Barley • Bran cereals • Couscous • Pistachios • Rye • Semolina • Sweets, Sweeteners and Spreads • Agavae • Fructose • High fructose corn syrup (HFCS) • Honey • Milk chocolate • Sugar free sweets • Inulin • Isomalt • Maltitol • Mannitol • Sorbitol • Xylitol • Prebiotic Foods • The follow items can be added to yoghurts, snack bars etc: • FOS – fructooligosaccharides • Inulin • Oligofructose • Drinks • Beer – if drinking more than one bottle • Dandelion tea • Fruit and herbal teas with apple added • Orange juice in quantities over 100ml • Rum • Sugar free fizzy drinks – such as diet coke • Sports drinks • Wine – if drinking more than one glass • Dairy Foods • Buttermilk • Cream cheese • Cream • Custard • Ice cream • Margarine • Milk – cow, goat and sheep • Sour cream • Yoghurt – including greek yogurt
Post-infectious IBS • 7-30 % of patients with a proven bacterial gastroenteritis will develop IBS. • Definition: PI-IBS is an acute Rome II criteria positive IBS developing after an infectious illness, characterised by two or more of the following: -fever -vomiting -acute diarrhoea -positive stool culture • PI-IBS: clinically distinct subgroup characterized by more diarrheal symptoms, less psychiatric illness, and increased serotonin-containing Enterochromaffin cells (EC cells) compared to those with non–PI-IBS. • unlike most other IBS there is a clearly defined start date
The pathogenesis of post-infectiousIrritableBowelSyndrome: • Inflammation increased production of serotonin by EC cells impairment of expression of SERT impaired clearance of serotoninfrom the gut • Consequences: - enhancedmotility - increasedintestinalpermeability - increasedsensitivity • Gut. 2002 Sep;51(3):410-3. • Prognosis in post-infectiveirritablebowelsyndrome: a sixyearfollow up study. • Neal KR, Barker L, Spiller RC.
IBS and the diagnosis positive diagnostic criteria vs. exclusion diagnosis? WRONG QUESTION: DIAGNOSIS IS ABOUT PROBABILITIES!
IBSClinical presentation and diagnosis To consider (depending on history, physical and mental examination, basic lab, and environment): • Postinfectious IBS (onset!) • Lactose intolerance • Other nutritional causes (fructose, BMI) • Chronic parasitic infection • Inflammatory Bowel Disease • Early childhood trauma • Psychosocial stress/events (chronic > acute)
IBSClinical diagnosis Useless: • Genetic testing • Explorative allergy testing • Extended microbiology of the faeces • Sophisticated motility tests (barostat) • Primary psychiatry consultation
IBSClinical presentation and diagnosis Useful: - Comorbidity (fibromyalgia; dyspepsia; dysuria; etc) - Assessment anxiety and depression (HADS) - Assessment Health-Related Quality of Life (HRQoL)
Relation between concurrent anxiety and/or depression and SF-36 Mean score SF-36 subscales
IBSTreatment Is there a standard treatment for IBS? NO (and YES)
IBSTreatment, some progress (1) Bijkerk et al. BMJ 2009; 339: b3154 “Soluble or insoluble fibre in irritable bowel syndrome in primary care? Randomised placebo controlled trial” Setting: General practice, Netherlands N= 275 Treatment: psyllium 10 g or bran 10 g or placebo 10 g Outcome: psyllium better than both alternatives, with the best symptom reduction after 3 months
IBSTreatment, some progress (2) Simren et al. Aliment Pharmacol Ther 2010; 31: 217-27 “Clinical trial: the effects of a fermented milk containing three probiotic bacteria in patients with irritable bowel syndrome, a randomized, double-blind, controlled trial” Setting: outpatient N= 74 Probiotic: 2 lactobacilli, 1 bifidobacter, in acidified milk Duration: 8 weeks; weekly assessment Response: probiotic 38%, placebo 27% (n.s.); probiotics better in the initial 2 weeks
The last meta-analysis • Am J Gastroenterol. 2014 Jul 29. doi: 10.1038/ajg.2014.202. [Epub ahead of print] • Efficacy of Prebiotics, Probiotics, and Synbiotics in Irritable Bowel Syndrome and Chronic Idiopathic Constipation: Systematic Review and Meta-analysis. • Ford AC1, Quigley EM2, Lacy BE3, Lembo AJ4, Saito YA5, Schiller LR6, Soffer EE7, Spiegel BM8, Moayyedi P9
Postinfectious IBSOutcome (1) Good hope: Jung et al. J Clin Gastroenterol 2009; 43: 534-40 “The clinical course of postinfectious irritable bowel syndrome: a five-year follow-up study” Setting: Hospital personnel; 5 years after Shigella infection outbreak N= 119 (Shigella exposed 60; controls 59) Follow-up at 1, 3, 5 years
Postinfectious IBSOutcome (2) IBS after infection (in %) Time Shigella + Shigella – 1 year 13,8 1.1 s. 3 years 14.9 4.5 s. 5 years 20.8 12.2 n.s.
IBSFuture needs (1) At short term: • Knowledge about causes and natural history • Capacity to apply a bio-psycho-social model to diagnosis, therapy and follow-up (SPECT) • Patient-orientated healthcare organisation • More public information about “functional” gastrointestinal disorders and their comorbidity
IBSFuture needs (2) At longer term, individualised care: • Markers for the pathogenetic contribution of Central and Peripheral Nervous System, gut flora and immune system, as well as for the psycho-social risks factors • Drugs and clinical techniques that can interfere at central, intermediate and/or peripheral levels