Download
1 / 66
680 likes | 740 Views
Prevalence of Keratoconus in Refractive Surgery Population in Sohag Governorate. Presented by Adham Salah El-Din Mohammed M.B., B.CH Assistant lecturer in Ophthalmology Department, Sohag Faculty of Medicine, Sohag University. سورة المجادلة – آية 11. Introduction. INTRODUCTION.

E N D
Prevalence of Keratoconus in Refractive Surgery Population in Sohag Governorate Presented by Adham Salah El-Din Mohammed M.B., B.CH Assistant lecturer in Ophthalmology Department, Sohag Faculty of Medicine, Sohag University
INTRODUCTION Introduction • Keratoconus (KC) is a developmental anomaly in which the inferior or central portion of the cornea becomes thinner and bulges forward in a cone-shaped fashion as a result of non-inflammatory thinning of the corneal stroma.
INTRODUCTION • The term keratoconus comes from the Greek words keras (horn) and konos (cone) and the condition has been known since the middle of the 19th century. • Most cases of keratoconus are bilateral, although usually asymmetric in severity and progression. In many cases, the disorder may start unilaterally, but eventually, the other eye becomes involved.
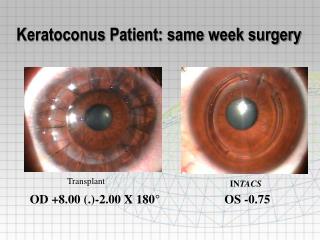
Aim of the Work Aim of the Work • To study the epidemiological state of keratoconus in people who are seeking refractive surgery; LASIK to correct their refractive errors, grades of the disease, common risk factors.
EPIDEMIOLOGY Epidemiology • Keratoconus is a relatively common disorder with a prevalence of 50 - 230/100,000. • Keratoconus affects all races and both sexes more or less equally. • Environmental factors may contribute to the wide variation in prevalence.
Risk Factors Risk Factors A) Environmental Factors 1. Eye Rubbing • An association between eye rubbing and KC has long been described and accepted as a risk factor. • Most authors report that about half of KC patients rub their eyes.
Risk Factors 2. Atopy • Atopyis a hypersensitivity reaction, which comprises allergy, asthma, and eczema. • It is found in about a third of KC patients, with variable percentage. 3. Sun Exposure • Ultraviolet light (UV) is a source of reactive oxygen species (ROS) and excessive exposure to sunlight leads to oxidative damage to KC corneas
Risk Factors B) Socioeconomic Factors 1. Age • KC Starts typically at the age of puberty, and usually continues over a period of next 10-20 years. • The process continues until the progression gradually stops.
Risk Factors 2. Geographic Location • Affect prevalence due to the different climate which influence the development of KC, • So, the Middle East, India and China reported higher rates than colder countries as Japan, northern Europe and USA.
Risk Factors C) Familial Factors: 1. KC in the Family • A large positive family history of the disease may occur due to either common environmental or genetic causes. 2. Consanguinity • A study made in 2000, proved that the genetic effect of consanguinity plays an important role in the pathogenesis of KC
Clinical Picture Clinical Picture • Symptoms • Early: asymptomatic. • Decreased visual acuity • Visual distortion. • Due to (Irregular astigmatism, myopia and corneal scarring)
Clinical Picture • Signs Clinical signs: 1- Munson’s sign
Clinical Picture 2- Rizzuti’s sign:
Clinical Picture • Retinoscopicsign: Scissor reflex
Clinical Picture • Direct Opthalmoscopysign Oil droplet sign
Clinical Picture • Slit lamp Biomicroscopic signs: Fleischer ring
Clinical Picture • Slit lamp Biomicroscopic signs: Vogt’s striae
Clinical Picture • Slit lamp Biomicroscopic signs: Prominent corneal nerves
Clinical Picture • Slit lamp Biomicroscopic signs: • Corneal Hydrops • Corneal scarring
Clinical Picture Pellucid Marginal Degeneration • A condition having the same biomechanical etiology as keratoconus, but the corneal thinning is in the far periphery close to the lower limbus. • It is considered a subtype of keratoconus.
Investigations Photokeratoscopy • The precursor of corneal topography. • It uses concentric rings (mires) called a placido disc with alternating bright and dark rings.
Investigations Corneal Topography • A sensitive method of assessing corneal shape. • It allows the early detection of subclinical “forme fruste” cases • produces a color-coded topographic map of the corneal surface and various numerical indices.
Investigations Corneal Hysteresis • It is the difference between the pressure at which the cornea bends inward and outward again after an air jet applanation. • It is used as an approach to keratoconus screening by measuring the bending resistance
Investigations • Cornea with regular astigmatism. B) Keratoconus (which shows lower • hysteresis values than normal cornea
Patients & Methods Patients and Methods • A prospective randomized clinical Study. • It was held in the Future center for LASIK and refractive surgery in Sohag. • 2000 eyes to 1202 patients (623 males and 579 females) were randomly chosen in the period from April to October 2015. • Screening was bilateral in 798 patients and unilateral in 404 patients.
Patients & Methods • Evaluation of the patient includes: A) History taking: • Sex • Age • State of consanguinity • Medical ophthalmological problem e.g. eye rubbing (counting the approximate attacks of eye allergy per year).
Patients & Methods B) Pentacam was done to all cases, and the following data were obtained: • Pachymetry (thinnest corneal location). • Keratometry (the steepest and flattest meridian of the cornea and the average Keratometry). • The posterior surface elevation.
Patients & Methods Grading of keratoconus: • Grade 0: subclinical keratoconus: with mean Keratometry <48D, pachymetry >500 um • Grade I: keratoconus with Keratometry 48 to less than 52 D, pachymetry 400-500 um • Grade II: keratoconus with Keratometry 52 to less than 55 D, pachymetry 200-400 um • Grade III: keratoconus with Keratometry more than 55 D, pachymetry <200 um, ± corneal scar.
There may be intersection or overlap between different categories of grades of keratoconus • Approval of scientific ethical committee was obtained before the start of the research.
Results Sex: • The resulting cases of keratoconus were 293 eyes (14.65%) of 210 patients. Of those patients, males were 117 (56.25%) and females were 93 (43.75%)
Results Age:
Results • Age was sub-divided into seven groups:
Results Eye allergy:
Results • Consanguinity:
Results Pachymetry
Results Keratometry