Download
1 / 47
490 likes | 925 Views
Adrenocorticosteroids And Adrenocortical antagonists. DR.Dr. Endang Isbandiati Soediono, MS, SpFK Dept.PharmacologyTherapy,MedicalFaculty,AirlanggaUniversit Dept.Clinical Pharmacology,Dr.Soetomo-Teaching Hospital, SURABAYA. ADRENAL CORTEX STEROID. Glucocorticoids Mineralocorticoids

E N D
Adrenocorticosteroids And Adrenocortical antagonists • DR.Dr. Endang Isbandiati Soediono, MS, SpFK • Dept.PharmacologyTherapy,MedicalFaculty,AirlanggaUniversit • Dept.Clinical Pharmacology,Dr.Soetomo-Teaching Hospital, • SURABAYA FKMPcoCorOADEIS09
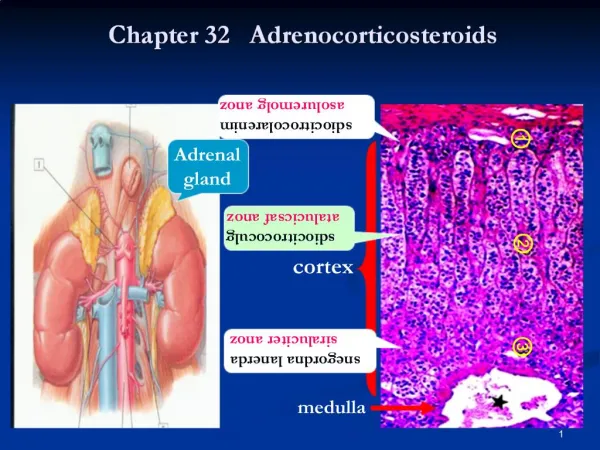
ADRENAL CORTEX STEROID • Glucocorticoids • Mineralocorticoids • Sex Steroids ( Androgen & Estrogen) • Human glucocorticoid : cortisol mineralocorticoid : aldosterone FKMPcoCorOADEIS09
HPA - AXIS FKMPcoCorOADEIS09
CIRCADIAN RHYTM FKMPcoCorOADEIS09
Mineralocorticoid Glucocorticoid Androgen ADRENALSTEROID BIOSYNTHESIS Testosterone Cortisol Aldosterone FKMPcoCorOADEIS09
CORTISOL Pharmacokinetic very sensitive to negative feedback cyrcadian rhythm (peak : early morning & after meal) Protein Binding (saturable) : CBG ( α2 – globulin 90%) albumin (5%) Pregnancy Hypothyroidism Estrogen CBG Genetic defect CBG Hyperthyroidism Protein deficiency FKMPcoCorOADEIS09
Cortisol continued Pharmacodynamic MOA : family of nuclear receptors (steroid, sterol, thyroid, retinoid acid) Physiological Effects: direct actions homeostatic responses “ permissive “ effects FKMPcoCorOADEIS09
C. Metabolic Effects Dose- related: carbohydrate, protein, fat fasted state muscle catabolism amino acid gluconeogenesis glycogen synthesis FKMPcoCorOADEIS09
glucocorticoidglucose insulin lipolysis lipogenesis fat deposition fatty acid glycerol FKMPcoCorOADEIS09
D. Catabolic Effects Hepar : protein & RNA synthesis Catabolic: lymphoid, connective tissue, muscle, fat, and skin Cushing’s syndrome bone osteoporosis Hi.Do. : muscle mass weakness Children : reduce growth FKMPcoCorOADEIS09
E. Anti-inflammatory & Immunosuppressive Effects Glucocorticoid Leukocytes PG Leukotriene PAF Mediators of inflammation (cytokine, chemokine, lipid, glucolipid) Anti-inflammation FKMPcoCorOADEIS09
F. Other Effects: . adrenal insufficiency psychiatric depression . glucocorticoid >>> insomnia, euphoria intracranial pressure depression FKMPcoCorOADEIS09
Chronic glucocorticoid:suppress the pituitary ACTH, GH, TSH, LH Hi.Do. : peptic ulcer Fat redis. : visceral, facial, nuchal& supraclav. Antagonize : Ca2+absorption Increase :platelet and red blood cells Cortisol (-) : impaired GFR, vasopressin Development of fetal lungs (surfactant) FKMPcoCorOADEIS09
CLINICAL PHARMACOLOGYA. Dx& Txof Disturbed Adrenal Function • AdrenocorticalInsufficiency • AdrenocorticalHypo- and Hyperfunction 3. Diagnostic purposes B. Stimulation of Lung MaturationHi.do. : prevent resp. distress in premature infant FKMPcoCorOADEIS09
C. Nonadrenal Disorders . Rheumatic Disorders . Hepatic disease . Noninflammatory joint dis. Malignancies . Renal diseases . Cerebral edema . Alergic disease . Sarcoidosis . Bronchial asthma . Thrombocytopenia . Infectious disease . Autoimmune destr. . Ocular disease of erythrocytes . Skin disease . Organ transpl. . Gastrointestinal disease . Spinal cord injury FKMPcoCorOADEIS09
Corticosteroid !!!!! • …to prevent damage from an inflammatory • Should not stopped abruptly • The shorter-acting glucocorticoid(Prednisone, Methylprednisolone) preferred to facilitate drug tapering and/or conversion to alternate-daytherapy • Considered : diet rich in potassium and low in sodium high protein intake antacid pts.epigastric distress Ca and vit. D FKMPcoCorOADEIS09
Toxicity • Metabolic Effects . fat tends to be redistributed to the trunk • Other Complication peptic ulcer masking bacterial and mycotic infection proximal myopathy hypomania or acute psychosis increase intraocular pressure pts heart dis. : sodium retention lead to CHF • Adrenal Suppression: tapering off FKMPcoCorOADEIS09
Contraindication & Caution A. Special precaution Monitore : hyperglycemia, glycosuria, sodium retention with edema/ HT, hypokalemia, peptic ulcer, osteoporosis B. Contraindications Peptic ulcer, heart disease / HT with CHF, infections, psychosis, diabetes, osteoporosis, glaucoma, herpes simplex infection FKMPcoCorOADEIS09
MINERALOCORTICOIDS(Aldosterone, Deoxycorticosterone, Fludrocortisone) • Aldosterone Promote the reabsorption of sodium Overdosage : hypernatremia, hypokalemia, metabolic alkalosis, increased plasma volume, HT • Deoxycorticosterone (DOC) A precursor of aldosterone Secretion is primarily under the control of ACTH • Fludrocortisone Both glucocorticoid and mineralocorticoid activity FKMPcoCorOADEIS09
ANTAGONIST OF ADRENOCORTICAL • METYRAPONE Inhibit 11- hydroxylation :cortisol& corticosterone Tx. : severe cortisolexcess AE : salt & water retention, hirsutism • AMINOGLUTETHIMIDE Tx. : (+) Dexamethasoneor Hydrocortisoneto < E (+) Metyraponeor Ketoconazoleto < steroid Increase clearance of Dexamethasone • KETOCONAZOLE Inhibitor of adrenal and gonadal steroid synthesis Tx. use : Cushing’s syndrome FKMPcoCorOADEIS09
ANTAGONIST OF ADRENOCORTICAL ( continued) • MIFEPRISTONE (RU 486) Blocks the glucocorticoidreceptors Tx. : inoperable ectopic ACTH secretion adrenal Ca Progesterone antagonist • MITOTANE adrenolytic toxic effects : n, v, d, depression, somnolence FKMPcoCorOADEIS09
MINERALOCORTICOID ANTAGONIST • SPIRONOLACTONE Interfere aldosteronesynthesis Tx. use : primary aldosteronism hirsutism in women diuretic CHF AE : hyperkalemia, Cardiaarr., menstrual abnorm., gynecomastia, sedation, GIT FKMPcoCorOADEIS09
PANCREATIC HORMONE And ANTIDIABETIC DRUGS FKMPcoCorOADEIS09
INSULIN • Secretion : low basal rate higher rate glucose sugar ( mannose) amino acids (leucine, arginine) vagal activity FKMPcoCorOADEIS09
Insulin lowers the concentration of BG a. inhibiting hepatic glucose production EC50 : ± 20 μU/ml b. stimulating the uptake and metabolism by muscle and adipose tissue EC50 : ± 50 μU/ml FKMPcoCorOADEIS09
The Insulin Receptors • Affinity : . hydrocortisone . Growth Hormone . insulin desensitization (obese; insulinoma) FKMPcoCorOADEIS09
Diabetes Mellitus Type 1 absolute deficiency of insulin immune-mediated idiopathic Environmental : infections, chemical, dietary Type 2 Heterogenous disorders : Insulin resistance & relative insulindeficiency or β - cell dysfunction FKMPcoCorOADEIS09
Blood Glucose Level . excessive glucagon . defect of somatostatin; excess of GH, cortisol, epinephrine . Drugs : corticosteroids, diazoxide, phenytoin, glucagon, caffein, cyclophosphamide, lithium, epinephrine, estrogens, furosemide, thiazide, thyroid prep., and sugar containing medication .sulfonylureas, disopyramide, ethanol, MAO-inhibitors, propranolol, and salicylates .Cushing’s disease, phaeochromocytoma, aldosteronism, hyperthyroidism, pancreatitis, cirrhosis, pregnancy, emotional stress, and infection FKMPcoCorOADEIS09
DM : Treatment • Non Pharmacologic Therapy: Diet & Activity • Pharmacologic Therapy • Insulin (as monotherapyin Type 1 DM) • Oral Anti Diabetic Agents: • . Sulfonylurea . Meglitinide • . Biguanide . Thiazolidinedione. Alpha- Glucosidase Inhibitor . Pramlintide • . Exenatide . Sitagliptin FKMPcoCorOADEIS09
Insulin : available preparations (1) Ultra-short –acting (Insulin Lispro) (2) Short- acting (Regular Insulin) Rapid onset of action (sc 30 min. and last 5 – 7 h) DOA; OOA : intensityof peak action > : dose > Short- acting soluble insulin : intravenous adm. (3) Intermediate and Long-acting (4) Mixtures FKMPcoCorOADEIS09
Complications of Insulin Therapy A. Hypoglycemia: Autonomic hyperactivity; Impaired CNS Treatment : . glucose . Uncosciousnessor stupor : 50% glucose iv/ 2-3 min 1mg glucagon sc/im B. Allergyand Resistance C. Lipoatrophy and lipohypertrophy D. Edema; abdominal bloating, and blurred vision. FKMPcoCorOADEIS09
Drug Interactions • Drug induced hypoglycemic states : ethanol, β - adrenergic receptor antagonists, salicylates, (pentamidine). • Drugs cause hyperglycemia : epinephrine, glucocorticoids phenytoin, clonidine, Ca channel-blocker K+ depletion FKMPcoCorOADEIS09
Oral Antidiabetic Agents .Insulin secretagogues : Sulfonylureas; Meglitinides; D-phenylalanine derv. . Biguanides . Thiazolidinediones . Alpha-glucosidaseinhibitors . Pramlintide . Exenatide . Sitagliptin FKMPcoCorOADEIS09
Sulfonylurea MOA A. Major action : increase insulin release B. Reduction of glucagon level C. Extrapancreatic effect FKMPcoCorOADEIS09
First Generation of Sulfonylurea Tolbutamide Prolonged hypoglycemia : (+) inhibition metabolism Dicumarol, Phenylbutazone, or Sulfonamide Chlorpropamide CI : hepatic and renal insufficiency Antidiuretic effect : (+) Tolazamide Doa shorter than chlorpropamide OOA: several hours FKMPcoCorOADEIS09
Second Generation of Sulfonylurea Glyburide, Glipizide, and Glimepiride potent sulfonylurea caution : CV diseases elderly FKMPcoCorOADEIS09
GLYBURIDE Metabolite : very low hypoglycemic activity CI : hepatic impairment and renal insufficiency Glipizide Absorption delayed when taken with food Less serious hypoglycemia CI : hepatic and renal insufficiency Glimepiride The lowest dose blood glucose lowering effect FKMPcoCorOADEIS09
Meglitinide MOA modulate β - cell insulin release ( potassium efflux ) Repaglinide : very fast ooa Adverse Effect : weight gain & hypoglycemia Interactions: Ketoconazole, Miconazole, Erythromycin: metabolism Carbamazepine, Barbiturates: metabolism FKMPcoCorOADEIS09
BIGUANIDE MOA Blood glucose lowering effect does not depend on the presence of functioning pancreatic β – cells …. “euglycemic “ / antihyperglycemic agent (1) direct stimulation of tissues glycolysis glucose removal from blood (2) Hepatic& renal gluconeogenesis (3) Slowing glucose absorption from GIT (4) Plasmaglucagon levels FKMPcoCorOADEIS09
Metabolism and Excretion Gluconeogenesis blockade: impair hepatic uptake of lactic ac. Renal insufficiency : lactic acidosis Clinical Use Refractory obesity, “insulin resistance syndrome” Combination with sulfonylurea CI : renal disease, alcoholism, hepatic disease, predisposing to tissue anoxia Adverse effects: abdom. bloating, diarrhea, nausea FKMPcoCorOADEIS09
THIAZOLIDINEDIONE Rosiglitazone and Pioglitazone MOA Glucose uptake and metabolism in muscle and adipose tissues Restrain gluconeogenesis, lipid metabolism, ovarian steroidogenesis, systemic blood pressure, and the fibrinolytic system … an “euglycemic” Chronic therapy : TG ; HDL and LDL Metabolized: cytochrome P450 Common AE : mild anemia FKMPcoCorOADEIS09
ALPHA- GLUCOSIDASE INHIBITOR Acarboseand Miglitol: competitive inhibitors of α – glucosidase . minimize upper intestinal digestion . defer digestion and absorption lowering postmealglycemic excursion ( insulin – sparing effect) FKMPcoCorOADEIS09
Adverse Effects Flatulence, diarrhea and abdominal pain Tolerance to the side effects : (+) Hypoglycemia : (+) insulin or sulfonylurea Treatment : glucose (dextrose) but not sucrose CI : serum creatinine > 2,0 mg/dL chronic or inflammatory bowel disease Caution : hepatic disease Interaction : intestinal adsorbent (charcoal) FKMPcoCorOADEIS09
Pramlintide • Antihyperglycemic (injectable) preprandial use Postprandial glucose (type 1 and type 2 DM ) MOA : suppresses glucagon release, delays gastric emptying, CNS anorectic Absorption : abdomen, thigh Injection : separate syringe FKMPcoCorOADEIS09
Exenatide • MOA : potensiated glucose-mediated insulin secretion, suppresseion of glucagon release, slowed gastric emptying, and CNS loss of appetite Sitagliptin • Renal impairment : dose adjustment • Hypoglycemic : rare • Facilitated weight loss FKMPcoCorOADEIS09
GLUCAGON Regulation of secretion : . glucose, insulin, amino acid, fatty acid, keton . Autonomic innervation DM : plasma glucagon gluconeogenesis & glycogenolysis hyperglycemia FKMPcoCorOADEIS09
THANK YOU FKMPcoCorOADEIS09