Download
1 / 17
240 likes | 690 Views
LIVER ABSCESS. Marc Richards Morning Report September 8th, 2009. CLASSIFICATIONS. PYOGENIC Gram Positive Gram Negative Anaerobic (Polymicrobial) AMEBIC CANDIDA TB (rare). EPIDEMIOLOGY. Pyogenic Abscesses Bacterial Most common M > F 3:1 Entamoeba M > F 7:1

E N D
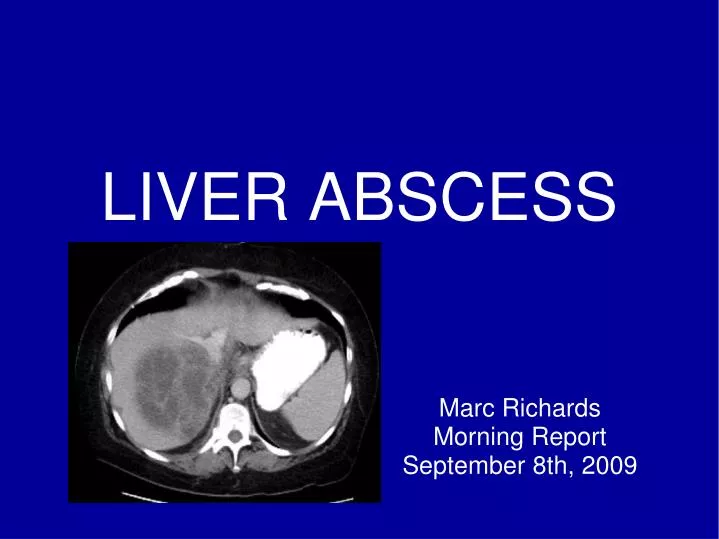
LIVER ABSCESS Marc Richards Morning Report September 8th, 2009
CLASSIFICATIONS PYOGENIC Gram Positive Gram Negative Anaerobic (Polymicrobial) AMEBIC CANDIDA TB (rare)
EPIDEMIOLOGY Pyogenic Abscesses Bacterial Most common M > F 3:1 Entamoeba M > F 7:1 40-50 million amoeba infections/year worldwide Age Extremes Endemic Areas most susceptible Country of origin or Travel
RISK FACTORS PYOGENIC DM Cancer Liver Transplant ENTAMOEBA Pregnancy Steroids Cancer Endemic area travel (short or long term) EtOH?
PATHOPHYS. PYOGENIC: Peritonitis To liver via portal circulation Direct Spread Biliary infections Hematogenous Seeding Look for bacteremia! Sites: R lobe most common Blood supply
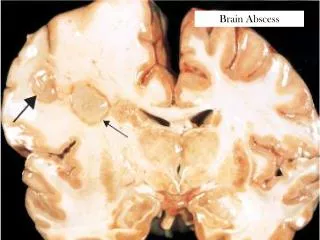
PATHOPHYS. ENTAMOEBA: Fecal-Oral transmission into GI Tract To liver via portal circulation Can also spread to other extraintestinal sites Heart Brain Lungs
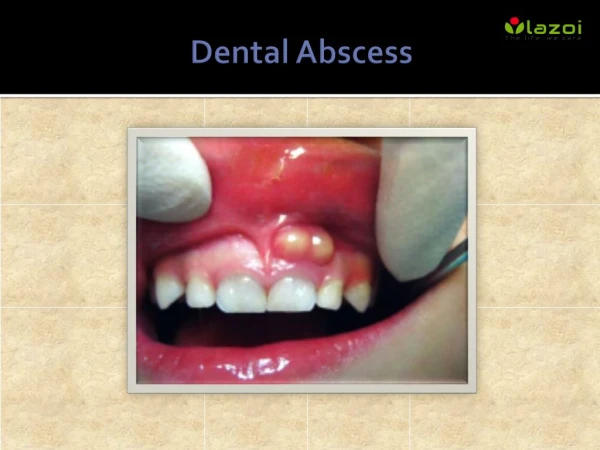
SIGNS • Hepatomegaly (50%) • RUQ tenderness • Jaundice • Acute abdomen (<7%) CLINICAL MANIFESTATIONS SYMPTOMS Fever (90%) RUQ pain (50-75%) Constitutional Sx Diarrhea (<30%)
WORKUP CBC (leukocytosis) LFTs AlkPhos elevated (67-90%) AST/ALT elevated (50%) TBili elevated (50%) Blood Cultures Bacteremia (50%) E Histolytica Ab Echinococcus Ab Imaging- US, CT, MRI Can not differentiate types of abscess
CT/MRI Fluid Collection w/ surrounding stranding, edema, and inflammation
DIAGNOSTIC PROCEDURE ***IMAGING-GUIDEDDRAINAGE*** • ***SEND FOR CULTURE***
WHAT MAY GROW… POLYMICROBIAL (including anaerobes) GRAM NEGATIVES (think gut bugs) E. Histolytica Money is in the serum Ab (95%) Less yield with wet-mount of abscess or fecal microscopy (<20%) OTHERS Strep Milleri group S Aureus (chemoembo) S Pyogenes (chemoembo) Candida (s/p chemo) Klebsiella TB Burkholderia
TREATMENT TO DRAIN OR NOT TO DRAIN: <5cm, single abscess- needle aspiration or catheter >5cm- catheter Also: Surgery, ERCP Amoeba: drainage not usually required Exceptions: Verge of rupture Abx not working Imminent need to exclude other dx
TREATMENT-ABX Pyogenic: Gram Neg + Anaerobe cov. Unasyn Zosyn 3rd gen Ceph (Rocephin) + Flagyl PCN Allergy: FQ + Flagyl, Carbapenem Course: 4-6 weeks IV duration depends on f/u imaging Suitable PO Abx: Augmentin OR FQ + Flagyl Amoeba: Flagyl 500-750mg TID 7-10days Then follow with lumenal antiamebic Usually Paromomycin TID 10d
PROGNOSIS & NATURAL HISTORY Mortality 2-12% Often due to comorbidities, not necessarily abscess itself
TAKE HOME MESSAGE Think Pyogenic (usually gram neg/anaerobe) or E.Histolytica Broad Spectrum Abx at first Image Image Image Imaging-Guided Culture +/- JP Drain Treat for 4-6 weeks MIAMI > FLORIDA STATE
REFERENCES eMedicine Current 2007 UpToDate Suki