Download
1 / 58
720 likes | 1.3k Views
PAIN SENSATION. By Dr FARAH AMIR ALI. Outline . Definition Purpose of pain Types of pain Difference b/w fast and slow pain Types of pain pathways Terminologies related to pain Analgesic system Thermoreceptor . PAIN: Definition:.

E N D
PAIN SENSATION By Dr FARAH AMIR ALI
Outline • Definition • Purpose of pain • Types of pain • Difference b/w fast and slow pain • Types of pain pathways • Terminologies related to pain • Analgesic system • Thermoreceptor
PAIN: Definition: • Pain refers to an unpleasant sensory and emotional experience associated with actual or potential tissue damage. • The word pain is from Greek word “POENA” means punishment or penalty.
Purpose of pain • Pain sensation is different from other sensations b/c its purpose is not to inform brain about quality of a stimulus, but rather to indicate that the stimulus is physically damaging. • Therefore, though pain is unpleasant , it is useful?
Purpose of pain • It makes one aware of a harmful agent in close contact with body. • It causes individual to react to remove the pain stimulus to prevent further damage. • Pain receptors are non-adapting, therefore , they keep the person apprised of damaging stimulus as long as it persists. thus the pain sensation has protective function
Types of pain • Qualitatively pain sensations are of two types: • FAST PAIN ( Good pain, physiologic pain, acute pain, sharp pain, pricking pain, electric pain) • SLOW PAIN ( Bad pain, pathologic pain, chronic pain, burning pain, aching pain, throbbing pain, nauseous pain)
FAST PAIN It is felt within 0.1 sec It is felt on superficial parts (Skin) SLOW PAIN It begins after 1 sec or more……even minutes It can occur in both in skin & in almost any deeper tissue or organ Difference b/w fast and slow pain
FAST PAIN 3) Receptors: FREE NERVE endings of Aσ fibers (6-30 m/s) Nature: Non adapting 4) Types of stimuli: Mechanical and thermal SLOW PAIN 3) Receptors FREE NERVE endings of C fibers (0.5-2 m/s) Nature: Non adapting 4) Types of stimuli Mechanical, thermal and chemical Difference b/w fast and slow pain
FAST PAIN 5)PATHWAY: Neospinothalamicpathway: 1st order neuron: terminate in lamina I (lamina marginalis) SLOW PAIN 5) PATHWAY Paleospinothalamicpathway 1st order neuron: terminate in lamina II & III (Substantia gelatinosa)…. then enter in Lamina V Difference b/w fast and slow pain
FAST PAIN 5)PATHWAY: Neospinothalamic pathway: 2nd order: crosses opposite side, travels upward in anterolateral pathway. A few fibers terminate in reticular formation, but most in ventrobasal complex. 3rd order to Somatosensory cortex SLOW PAIN 5) PATHWAY Paleospinothalamicpathway 2nd order: crosses opposite side, travels upward in anterolateral pathway . most widely terminate in reticular formation, only 1/10th directly to thalamus. Difference b/w fast and slow pain
FAST PAIN 5)PATHWAY: SLOW PAIN 5) PATHWAY Paleospinothalamicpathway 2nd order: most widely terminate in i)reticular nuclei of the medulla, pons & mesencephalon. ii) tectal area of mesencephalon iii) periaqueductal gray region) Difference b/w fast and slow pain
FAST PAIN Capability of localization of pain The fast-sharp type of pain can be localized much more exactly in the different parts of the body than can slow-chronic pain. Glutamate, the Probable Neurotransmitter of the Type A delta Fast Pain Fibers. SLOW PAIN Capability of localization of pain Very Poor Capability of the Nervous System to Localize Precisely the Source of Pain Transmitted in the Slow-Chronic Pathway. Substance P, the Probable Slow-Chronic Neurotransmitter of Type C Nerve Endings. Difference b/w fast and slow pain
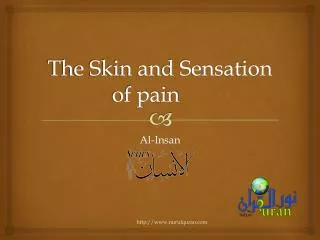
Transmission of both “fast-sharp” and slow-chronic” pain signals into and through the spinal cord on their way to the brain
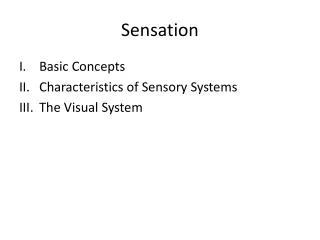
Transmission of pain signals into the brain stem, thalamus, and cerebral cortex by way of the fast pricking pain pathway and the low burning pain pathway
Function of the Reticular Formation, Thalamus, and Cerebral Cortex in the Appreciation of Pain. • Complete removal of the somatic sensory areas of the cerebral cortex does not destroy an animal’s ability to perceive pain. • pain impulses entering the brain stem reticular formation, the thalamus, and other lower brain centers cause conscious perception of pain.
Special Capability of Pain Signals to Arouse Brain Excitability • This explains why it is almost impossible for a person to sleep when he or she is in severe pain. Special Capability of Pain Signals to Arouse Overall Brain Excitability Special Capability of Pain Signals to Arouse Overall Brain Excitability
Terminologies related to pain • Referred pain: Pain which originates due to irritation of visceral organ and is not felt in the organ but in some other somatic structure (usually skin) supplied by same neuronal segment. Such pain is said to be referred to the second structure. Pain is usually referred to structure with common embryonic origin and hence are innervated by a common neuronal segment. This principle is called Dermatomal rule.
Referred pain…….. • For example, embryologicaly heart and left arm have same segmental origin. Similarly, the testes and kidney develop from same primitive urogenital ridge.
Referred pain…….. convergence–projection theory • The basis for referred pain may be convergence of somatic and visceral pain fibers on the same second-order neurons in the dorsal horn that project to the thalamus and then to the somatosensory cortex .This is called the convergence–projection theory
Headache • Headaches are a type of pain referred to the surface of the head from deep head structures. • Headache of Intracranial Origin: • Pain-Sensitive Areas in Cranial Vault. The brain tissues themselves are almost totally insensitive to pain.
Pain-Sensitive Areas in Cranial Vault • Conversely, tugging on the venous sinuses around the brain, damaging the tentorium, or stretching the dura at the base of the brain can cause intense pain that is recognized as headache.
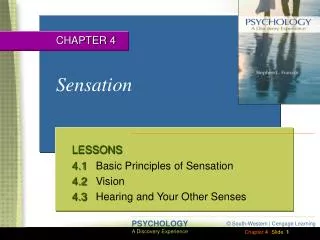
Areas of the Head to Which Intracranial Headache Is Referred
Types of Intracranial Headache • Headache of Meningitis • Headache Caused by Low Cerebrospinal Fluid Pressure • Migraine Headache • Alcoholic Headache • Headache Caused by Constipation
Extracranial Types of Headache • Headache Resulting from Muscle Spasm • Headache Caused by Irritation of Nasal and Accessory Nasal Structures • Headache Caused by Eye Disorders
Dermatomes • Each spinal nerve innervates a “segmental field” of the skin called a dermatome • the anal region of the body lies in the dermatome of the most distal cord segment, dermatome S5.
Dermatomes • In the embryo, this is the tail region and the most distal portion of the body. • The legs originate embryologically from the lumbar and upper sacral segments (L2 to S3), rather than from the distal sacral segments, which is evident from the dermatomal map.
Hyperalgesia and allodynia • Hyperalgesia is an exaggerated response to a noxious stimulus, • whereas allodynia is a sensation of pain in response to an harmless stimulus. (painful sensation from a warm shower when the skin is damaged by sunburn)
Neuropathic pain • Neuropathic pain may occur when nerve fibers are injured. Commonly, it is excruciating and a difficult condition to treat. • It occurs in various forms in humans. For example, in causalgia, spontaneous burning pain occurs long after seemingly trivial injuries.
Neuropathic pain • Research in animals indicates that nerve injury leads to sprouting and eventual overgrowth of noradrenergic sympathetic nerve fibers into the dorsal root ganglia of the sensory nerves from the injured area.
In response to tissue injury, chemical mediators can sensitize and activate nociceptors • Tissue injury releases bradykinin and prostaglandins that sensitize or activate nociceptors, which in turn releases substance P . • Substance P acts on mast cells to cause degranulation and release histamine, which activates nociceptors.
In response to tissue injury, chemical mediators can sensitize and activate nociceptors • Substance P causes plasma extravasation the resulting edema causes additional release of bradykinin. • Serotonin (5-HT) is released from platelets and activates nociceptors.
Visceral pain • Often, the viscera have sensory receptors for no other modalities of sensation besides pain. • Difference b/w somatic and visceral pain? • One of the most important differences between surface pain and visceral pain is that highly localized types of damage to the viscera seldom cause severe pain.
Visceral pain…….. • Causes: • Ischemia • Chemical stimuli • Spasm of hollow viscera • Overdistension of hollow viscera
Insensitive viscera • A few visceral areas are almost completely insensitive to pain of any type. • These include the parenchyma of the liver and the alveoli of the lungs.
Insensitive viscera • the liver capsule is extremely sensitive to both direct trauma and stretch, and the bile ducts are also sensitive to pain. • In the lungs, even though the alveoli are insensitive, both the bronchi and the parietal pleura are very sensitive to pain.
Occasionally herpesvirus infects a dorsal root ganglion. This causes severe pain in the dermatomal segment subserved by the ganglion, thus eliciting a segmental type of pain that circles halfway around the body. The disease is called herpes zoster, or “shingles,” because of a skin eruption that often ensues. . Herpes Zoster (Shingles)
Lancinating pain occasionally occurs in some people over one side of the face in the sensory distribution area (or part of the area) of the fifth or ninth nerves; this phenomenon is called tic douloureux (or trigeminal neuralgia or glossopharyngeal neuralgia). The pain feels like sudden electrical shocks, and it may appear for only a few seconds at a time or may be almost continuous. Tic Douloureux
If the spinal cord is transected entirely, all sensations and motor functions distal to the segment of transection are blocked, If the spinal cord is transected on only one side, the Brown-Séquard syndrome occurs. Brown-Séquard Syndrome
In Brown-Séquard syndrome all motor functions are blocked on the side of the transection in all segments below the level of the transection. The sensations of pain, heat, and cold sensations served by the spinothalamic pathway—are lost on the opposite side of the body in all dermatomes two to six segments below the level of the transection. Brown-Séquard Syndrome
By contrast, the sensations that are transmitted only in the dorsal and dorsolateral columns—kinesthetic and position sensations, vibration sensation, discrete localization, and two-point discrimination—are lost on the side of the transection in all dermatomes below the level of the transection. Brown-Séquard Syndrome
Pain Suppression (“Analgesia”) System in the brain and Spinal Cord • The degree to which a person reacts to pain varies tremendously. This results partly from a capability of the brain itself to suppress input of pain signals to the nervous system by activating a pain control system, called an analgesia system.
The analgesia system. Itconsists of three major components: (1) The periaqueductal gray and periventricular areas of the mesencephalon and upper pons surround the aqueduct of Sylvius and portions of the third and fourth ventricles. Neurons from these areas send signals to. Analgesic system…. Pathway descending ….
The analgesia system. Itconsists of three major components: (2) the raphe magnus nucleus, a thin midline nucleus located in the lower pons and upper medulla, and the nucleus reticularis paragigantocellularis, located laterally in the medulla. Analgesic system…. Pathway descending ….
Analgesic system…. Pathway descending …. • From these nuclei, second-order signals are transmitted down the dorsolateral columns in the spinal cord to (3) a pain inhibitory complex located in the dorsal horns of the spinal cord. At this point, the analgesia signals can block the pain before it is relayed to the brain.
Brain’s Opiate System—Endorphinsand Enkephalins • More than 35 years ago it was discovered that injection of minute quantities of morphine either into the periventricular nucleus around the third ventricle or into the periaqueductal gray area of the brain stem causes an extreme degree of analgesia • Therefore, an extensive search was undertaken for the natural opiate of the brain. About a dozen such opiate-like substances have now been found at different points of the nervous system;
Brain’s Opiate System—Endorphinsand Enkephalins • all are breakdown products of three large protein molecules: proopiomelanocortin, proenkephalin, and prodynorphin. • Among the more important of these opiate-like substances are b-endorphin, met-enkephalin, leuenkephalin, and dynorphin.