Download
1 / 62
640 likes | 1.08k Views
The program will start promptly at 10:00 AM. For technical assistance please contact Tech Support at 404-969-0387 or email at support@healthtecdl.org. Assessment of Fecal Incontinence and Constipation in the Female Patient. Mahmoud Barrie, MD Assistant Professor

E N D
The program will start promptly at 10:00 AM For technical assistance please contact Tech Support at 404-969-0387 or email at support@healthtecdl.org
Assessment of Fecal Incontinence and Constipation in the Female Patient Mahmoud Barrie, MD Assistant Professor Department of Gastroenterology/Hepatology Atlanta VAMC/EUH Atlanta, GA December 9, 2008 For technical assistance please contact Tech Support at 404-969-0387 or email at support@healthtecdl.org
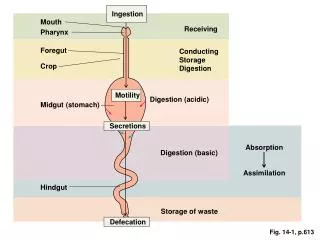
Outline Anatomy- Anorectum Mechanism of continence Fecal incontinence Epidemiology, etiology, clinical presentation Diagnostic studies Assessment Algorithm Mechanism of defecation Constipation Epidemiology, etiology, clinical presentation Diagnostic studies Assessment Algorithm Summary If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Objectives Anatomy- Anorectum Mechanism of continence Fecal incontinence Epidemiology, etiology, clinical presentation Pertinent radiographic and non-radiographic testing Mechanism of defecation Constipation Epidemiology, etiology, clinical presentation Pertinent radiographic and non-radiographic testing Summary If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
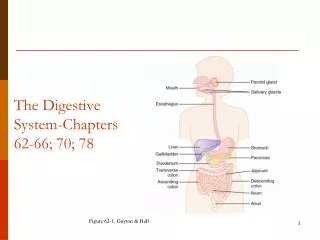
Epithelial nerve endings of the rectum and anus If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Anorectal function Continence Defecation If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Continence mechanisms Anorectal angle Rectal accomodation/compliance Rectal sensation Anal sensory nerves Internal anal sphincter External anal sphincter If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Continence Mechanisms: Anorectal Angle If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Continence Mechanisms: Rectal Accommodation If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Continence Mechanisms: Compliance Ratio of pressure to volume at different volumes of distention Decreased compliance with Inflammation Fibrosis Surgical replacement with sigmoid colon If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Continence Mechanisms: Rectal Compliance If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Fecal Incontinence Continuous or recurrent passage of fecal material (>10ml) for at least one month in a person older than 3/4 years of age If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Epidemiology A US study of outpatients found an overall prevalence of 18·4% Incontinence occurred daily in 2·7% of patients, weekly in 4·5%, and monthly or less in 7·1% Symptomatic fecal incontinence occurs in 21% of women presenting with urinary incontinence, pelvic-organ prolapse, or both If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Causes of Fecal Incontinence If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
A greater proportion of cases of faecal incontinence are acquired Sphincter disruption resulting from vaginal delivery= most common sphincter injury Sphincter atrophy due to advanced age If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Vaginal delivery injury risks Forceps delivery Primiparous: giving birth to a baby weighing over 4 kg- Traction injury to the pudendal nerve third-degree obstetric lacerations Incidence of both flatus and stool: 6-25% in new postpartum 3-27% in known sphincter tears If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Assessment Essential elements of the history: Onset Type of incontinence (flatus, liquid, or solid stool) Frequency of episodes Pertinent findings in the physical exam include: A thinned or deformed perianal body and scars from previous surgery or trauma. Breakdown of the perianal skin is a consequence, not a cause of incontinence Gaping of the anus suggests rectal prolapse, which can usually be demonstrated with Valsalva’s manoeuvre. Diminished perianal sensation and the absence of an anal wink suggest a neurogenic cause Digital exam- weak sphincter squeeze If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Diagnostic Studies Function Anorectal manometry EMG: Action potentials of sphincter muscle PNTL Defecography: anorectal angle, perineal descent Anatomy Flexible sigmodoscopy/proctosocpy Defecography: rectoceles Anal sonography: Sphincter defect Barium enema MRI If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Function: Anorectal manometry in fecal incontinence If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Function: EMG Electromyography — Electromyography of the external anal sphincter and pelvic floor muscles is performed for three purposes: To identify areas of sphincter injury by mapping the sphincter. To determine whether the muscle contracts or relaxes (by the number of motor units firing). To identify denervation-reinnervation potentials indicative of nerve injury. If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Function: EAS EMG If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Function: EAS EMG Nerve sprouting Variations of intervals b/w motor unit potentials If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Function: Pudendal n. Latency If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Child Birth Neurologic evidence PNTL prolongation 42% of postpartum women (Snooks et al ) cesarean delivery performed in late labor (cervical dilation 8 cm or greater) EMG of the anal sphincter: increased fiber density in multiparous women(Allen RE et al.) If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Anatomy: Defecography Evacuation proctography: process, rate and completeness Assessing ano-rectal angle Structural and functional alterations: rectocele, internal rectal intussusception, external rectal prolapse, enterocele and pelvic floor dysfunction, or dyssynergia. If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Anatomy: Rectal Ultrasound If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Anatomy: Endoanal Coil MRI Sphincter atrophy 89% sensitivity 94% specificity 89% positive predictive value 94% negative predictive value Defect(atrophy) in levator ani m. May not be as good in detecting sphincter tear. If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Anatomic evidence Endoanal MRI: 20% of primiparous women: defect in the levator ani muscle (Delancey et al ) Endoanal ultrasound for sphincter disruption (Abramowitz L et al) 35% of primiparous 44% of multiparous If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Summary of diagnostic studies Anorectal manometry: Good EMG/PNTML: good but limited to specialized centers Defecography: Not as good Anal endosonography good Endoanal Coil MRI : New and promising If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Constipation Straining ≥1/4 of defecation; Lumpy or hard stools ≥1/4 of defecation; Sensation of incomplete defecation ≥1/4 of defecation; Sensation of anorectal obstruction/blockage≥1/4 of defecation; Manual maneuvers to facilitate ≥1/4 of defecation (example: digital evacuation, support of the pelvic floor); Less than three defecations per week. If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Epidemiology Prevalence 2-34% F:M 3 to 5x Increase >65yo If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Types of constipation Normal transit and normal pelvic floor function Slow transit (colonic inertia) Dyssynergic or obstructive defecation or anismus Structural abnormalities: Enteroceles and Rectoceles If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Assessment of Constipation H&P digital dysimpaction, pelvic and/back pain, bleeding, urinary incontinence, renal insufficiency Colonic scintigraphy Anorectal manometry/Balloon expulsion Surface EMG Evacuation proctography If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Colonic transit If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Balloon Expulsion If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org
Rectal pressure & EMG in PFD If you have any technical issues, please contact 404-969-0387 or email support@healthtecdl.org