Download
1 / 1
10 likes | 106 Views
No. 090. Predicting disease p rogression in pelvic Lymph Node (LN ) positive p atients a fter r adical p rostatectomy. Annah Vollstedt 1 , Laila Dahmoush 2 , Joseph Gillespie 3 , Anna Button 4 , Michael Henry 5 , James Brown 3

E N D
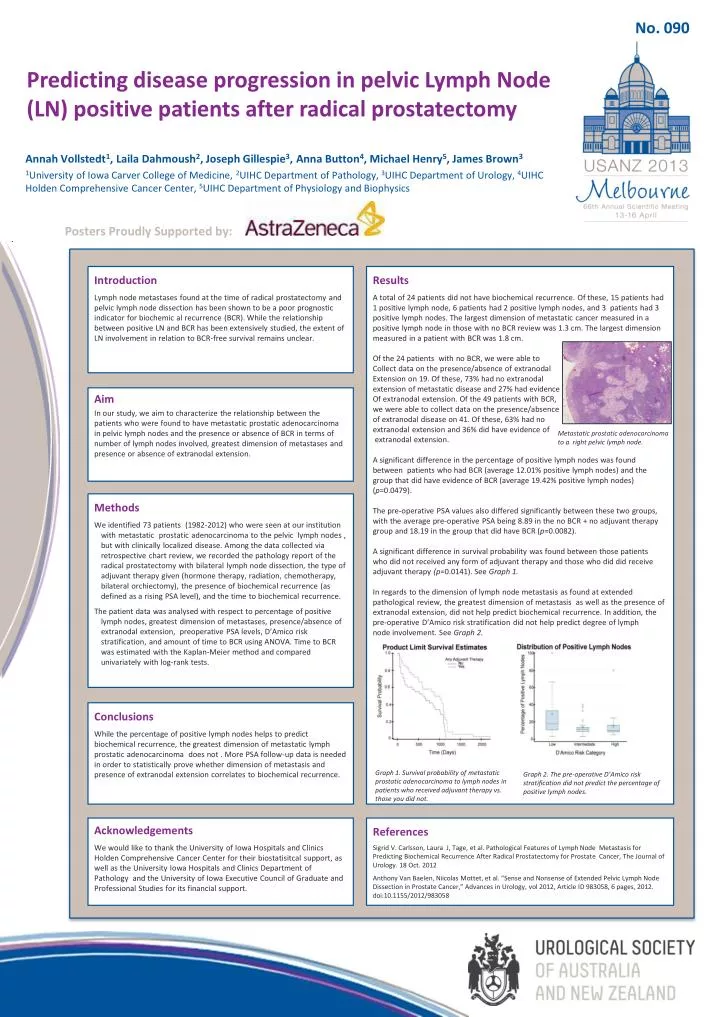
No. 090 Predicting disease progression in pelvic Lymph Node (LN) positive patients after radical prostatectomy Annah Vollstedt1, Laila Dahmoush2, Joseph Gillespie3, Anna Button4, Michael Henry5, James Brown3 1University of Iowa Carver College of Medicine, 2UIHC Department of Pathology, 3UIHC Department of Urology, 4UIHC Holden Comprehensive Cancer Center, 5UIHC Department of Physiology and Biophysics Posters Proudly Supported by: Introduction Lymph node metastases found at the time of radical prostatectomy and pelvic lymph node dissection has been shown to be a poor prognostic indicator for biochemic al recurrence (BCR). While the relationship between positive LN and BCR has been extensively studied, the extent of LN involvement in relation to BCR-free survival remains unclear. Results A total of 24 patients did not have biochemical recurrence. Of these, 15 patients had 1 positive lymph node, 6 patients had 2 positive lymph nodes, and 3 patients had 3 positive lymph nodes. The largest dimension of metastatic cancer measured in a positive lymph node in those with no BCR review was 1.3 cm. The largest dimension measured in a patient with BCR was 1.8 cm. Of the 24 patients with no BCR, we were able to Collectdata on the presence/absence of extranodal Extensionon 19. Of these, 73% had no extranodal extension of metastatic disease and 27% had evidence Ofextranodalextension. Of the 49 patients with BCR, we were able to collect data on the presence/absence of extranodal disease on 41. Of these, 63% had no extranodalextension and 36% did have evidence of extranodal extension. A significant difference in the percentage of positive lymph nodes was found between patients who had BCR (average 12.01% positive lymph nodes) and the group that did have evidence of BCR (average 19.42% positive lymph nodes) (p=0.0479). The pre-operative PSA values also differed significantly between these two groups, with the average pre-operative PSA being 8.89 in the no BCR+ no adjuvant therapy group and 18.19 in the group that did have BCR (p=0.0082). A significant difference in survival probability was found between those patients who did not received any form of adjuvant therapy and those who did did receive adjuvant therapy (p=0.0141). See Graph 1. In regards to the dimension of lymph node metastasis as found at extended pathological review, the greatest dimension of metastasis as well as the presence of extranodal extension, did not help predict biochemical recurrence. In addition, the pre-operative D’Amico risk stratification did not help predict degree of lymph node involvement. See Graph 2. Aim In our study, we aim to characterize the relationship between the patients who were found to have metastatic prostatic adenocarcinoma in pelvic lymph nodes and the presence or absence of BCRin terms of number of lymph nodes involved, greatest dimension of metastases and presence or absence of extranodal extension. Metastatic prostatic adenocarcinoma to a right pelvic lymph node. Methods We identified 73 patients (1982-2012) who were seen at our institution with metastatic prostatic adenocarcinoma to the pelvic lymph nodes , but with clinically localized disease. Among the data collected via retrospective chart review, we recorded the pathology report of the radical prostatectomy with bilateral lymph node dissection, the type of adjuvant therapy given (hormone therapy, radiation, chemotherapy, bilateral orchiectomy), the presence of biochemical recurrence (as defined as a rising PSA level), and the time to biochemical recurrence. The patient data was analysed with respect to percentage of positive lymph nodes, greatest dimension of metastases, presence/absence of extranodal extension, preoperative PSA levels, D’Amico risk stratification, and amount of time to BCR using ANOVA. Time to BCR was estimated with the Kaplan-Meier method and compared univariately with log-rank tests. Conclusions While the percentage of positive lymph nodes helps to predict biochemical recurrence, the greatest dimension of metastatic lymph prostatic adenocarcinoma does not . More PSA follow-up data is needed in order to statistically prove whether dimension of metastasis and presence of extranodal extension correlates to biochemical recurrence. Graph 1. Survival probability of metastatic prostatic adenocarcinoma to lymph nodes in patients who received adjuvant therapy vs. those you did not. Graph 2. The pre-operative D’Amico risk stratification did not predict the percentage of positive lymph nodes. Acknowledgements We would like to thank the University of Iowa Hospitals and Clinics Holden Comprehensive Cancer Center for their biostatisitcal support, as well as the University Iowa Hospitals and Clinics Department of Pathology and the University of Iowa Executive Council of Graduate and Professional Studies for its financial support. References Sigrid V. Carlsson, Laura J, Tage, et al. Pathological Features of Lymph Node Metastasis for Predicting Biochemical Recurrence After Radical Prostatectomy for Prostate Cancer, The Journal of Urology. 18 Oct. 2012 Anthony Van Baelen, NiicolasMottet, et al. “Sense and Nonsense of Extended Pelvic Lymph Node Dissection in Prostate Cancer,” Advances in Urology, vol 2012, Article ID 983058, 6 pages, 2012. doi:10.1155/2012/983058






