Download
1 / 22
260 likes | 646 Views
Cytotoxic Chemotherapy, Somatostatin Analogs and PRRT in NEC: Why, When and How to give?. Manisha H. Shah, M.D. Associate Professor of Internal Medicine The Ohio State University Comprehensive Cancer Center manisha.shah@osumc.edu. Outline. Agents: Somatostatin Analogs Cytotoxic Chemotherapy

E N D
Cytotoxic Chemotherapy, Somatostatin Analogs and PRRT in NEC: Why, When and How to give? Manisha H. Shah, M.D.Associate Professor of Internal MedicineThe Ohio State UniversityComprehensive Cancer Centermanisha.shah@osumc.edu
Outline Agents: • Somatostatin Analogs • Cytotoxic Chemotherapy • Peptide Receptor Radionuclide Therapy (PRRT) Points to discuss: • Why to give: Evidence for its use • When to give: Indications • How to give: Regimen details and toxicity
Somatostatin Analogs • Somatostatin: • 14 AA peptide made in D-cells of pancreas • Growth inhibiting in vitro • 5 Receptors cloned (ssrt 1-5) • Abundance of ssrt2 on carcinoid, islet cell • Octreotide (Sandostatin): • Short acting: Octreotide SQ TID (IV drip for crisis) • Long acting: Octreotide LAR IM once a month • Approved for carcinoid, VIPoma, acromegaly • Lanreotide (Somatuline): • Short acting: Lanreotide LA IM every 10-14 days • Long acting: Lanreotide depot SQ once a month • Approved for acromegaly • Pasireotide (SOM-230): Investigational
Octreotide: Why to give? • Carcinoid Syndrome: • Numerous phase II-III studies showing dramatic effectiveness of octreotide in controlling carcinoid syndrome symptoms • FDA approval for pts with carcinoid syndrome • Treatment of carcinoid tumor/Tumor stabilizing effect • Several phase II studies showing increase in time to progression • PROMID: Phase III study • No definitive studies showing control of tumors in in pts with pancreatic NET • No role in adjuvant setting
Octreotide: Why to give for Anti-tumor activity PROMID study: Phase III placebo controlled multicenter trial in Germany • Sample size 85 • Enrollment over 7 years (2001-2008) • midgut metastatic WDNEC (Ki-67 <2%) • treatment naïve • 75% of pts had liver tumor burden <10% • 38% pts had carcinoid syndrome • 4.3 months median time since dx to study Rinke et al, J Clin Oncol, 2009
Is statistically significant increase in median PFS (octreotide LAR vs placebo) clinically meaningful? PROMID study Interim analysis Median PFS 14.3 vs 6 months (octreotidevs placebo) P=.000072 Issues and Take Home Message: • How to explain median PFS of 6 months in placebo in low risk group • Indications are broadened to all comers with carcinoid • Consider following when recommending: • $$ factor, side effects, status of tumor burden, concurrent treatment
Octreotide: When to give? Treatment of hormone related symptoms • Carcinoid syndrome • Zollinger Ellison syndrome • VIPoma Tumor stabilizing effect • Metastatic carcinoid tumor Prevention and treatment of carcinoid crisis • Before surgery or procedures (stent change, dental, TACE) No role in adjuvant setting
Octreotide: How to give • For Carcinoid syndrome or Tumor stabilizing effect • Octreotide 100-200 mcg SQ TID x 7-10 d, if response, convert to long acting octreotide LAR 20-30 mg IM every weeks. • Higher or frequent doses of SQ octreotide or Continuous SQ infusion in severe uncontrolled carcinoid syndrome. • Titrate dose of octreotide LAR 40 mg or frequency to every 3 weeks • For prevention or treatment of Carcinoid crisis • octreotide before surgery or procedures • IV drip 35 mcg/hour titrate up prn
Octreotide: Monitoring for Side effects • Common: • Diarrhea (36%) • Abdominal discomfort (29%) • Flatulence (25%) • Constipation (19%) • Nausea (10%) • Gall stones, biliary sludge, jaundice (62% over 18 months therapy) • Hypoglycemia/Hyperglycemia • Hypothyroid • Rare/dangerous: • Sinus bradycardia or AV heart block
Octreotide: Monitoring and treatment of side effects • Check TSH once-twice a year • Evaluate GI symptoms: • Flatulence, steatorrhea • Treat with pancrelipase enzymes (creon 6000-24000 units) 1-2 tabs with every meal, snacks • Constipation: • Result of decreased bowel motility • Decrease or discontinue octreotide • Gall bladder stones
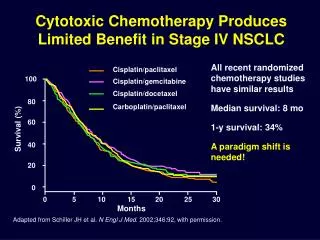
Cytotoxic chemo: Why to give? • Modest responses in pancreatic NET (Islet cell) • Streptozocin, doxorubicin (Moertel CG et al, N Engl J Med 1992): 125 pts prospective ECOG study • 69% response (any tumor shrinkage) • Median time to progression: 20 months • Streptozocin, 5 FU, Doxorubicin (Kouvaraki MA et al, J Clin Oncol 2004): 84 pts retrospective MD Anderson • 39% Partial responses • Median duration of response: 9.3 months • Temozolamide, capecitabine (Strosberg JR et al, Cancer 2010): 30 pts retrospective Moffitt Cancer Center • 70% Partial responses • Median PFS: 18 months • Little or no responses in Carcinoid tumors
Cytotoxic Chemo: When to give? Treatment of pNET (islet cell) • Progressive metastatic • Widespread nature/extra-hepatic mets • Unresectable liver mets • Locally Advanced (?Neo-adjuvant) No role in Carcinoid tumors • Exploratory • Etoposide/cisplatin based chemo should NOT be given in typical carcinoid even for pts who have aggressive clinical course No role in adjuvant setting in all NET
Cytotoxic Chemo: How to give? • Streptozocin/Doxorubicin: 6-wk cycle • Streptozocin 500 mg/m2 IV daily for 5 days • Doxorubicin 50 mg/m2 IV days 1 and 22 (cumulative max dose of 500 mg/m2) • 5FU/Doxorubicin/Streptozocin: 28 day cycle • Streptozocin 400 mg/m2 IV days 1-5 • 5FU 400 mg/m2 IV bolus days 1-5 • Doxorubicin 40 mg/m2 IV day 1 • Temozolomide/Capecitabine: 28 day cycle • Capecitabine 750 mg/m2 per dose PO BID, days 1-14 • Temozolomide 200 mg/m2 PO QD, days 10-14
Cytotoxic chemo: Side effects • Conventional: • Fatigue, nausea, vomiting, diarrhea, mucositis, cytopenias, infection • Cardiomyopathy (Doxo) • Renal toxicity (Strepto) • Unique side effects of tem/capecitabine • CNS: somnolence, memory issues, ataxia • Cytopenias: Sudden onset of severe thrombocytopenia (platelet count of 10-20K)
PRRT: Background • Peptide Receptor Radionuclide Therapy (PRRT) • Systemic radiotherapy • Radiolabeled Somatostatin analogs • Two potent agents • 177Lu-octreotate • 90Y-octreotide • Availability • Not available in US on/off trial • Tested and available in Europe x >10 years (many countries)
PRRT: Why to give? Schmidt et al, Oncogene, 2011
PRRT: When to give? Positive octreoscan is mandatory Treatment of Carcinoid and pNET (islet cell) • Progressive metastatic • Widespread nature/extra-hepatic mets • ?Before or after medical therapies Comparison to other systemic therapies • One of the best systemic therapies for carcinoid tumors • Very effective for pNET Factors affecting recommendation availability, feasibility of travel, expense No role in adjuvant setting in all NET
PRRT: How to give? • Will not give technical details • Has to be done in hands of experts: Referral to European centers (Emails, websites) • Systemic IV infusion • Supportive care with amino acid infusion • Schedule evolving from once every 6 weeks x 4 to now once every 6 months
PRRT: Side effects • Overall very well tolerated • Acute: • Fatigue, nausea, vomiting, cytopenias • Rare • Renal insufficiency • Myelodysplastic syndrome • ?Liver toxicity • Pts with high tumor burden, findings of liver cirrhosis/portal HTN
Take-Home Message (1) • Octreotide is VERY effective for control of carcinoid syndrome and also has a role in tumor stabilization in pts with mid gut carcinoid tumors • Cytotoxic chemo has modest activity in pts with pNET but NO activity in pts with carcinoid tumors • PRRT is one of the best systemic therapies for carcinoid tumors and also very effective in pts with pNET
Take-Home Message (2) • There is no role of adjuvant octreotide, chemo or PRRT • Etoposide/platinum based chemo should NOT be given in pts who have typical (well differentiated) carcinoid tumors even if they have aggressive clinical course • Clinical trials should be encouraged in all pts with NET
Thank You & Happy Holidays!