Download
1 / 50
560 likes | 1.31k Views
Zenker’s and Epiphrenic Diverticula. David W Rattner, MD Massachusetts General Hospital. Pharyngoesophageal diverticula. Pathogenesis of Zenker’s Diverticulum. Cricopharyngeus spasm caused by GER

E N D
Zenker’s and Epiphrenic Diverticula David W Rattner, MD Massachusetts General Hospital
Pathogenesis of Zenker’s Diverticulum • Cricopharyngeus spasm caused by GER • unclear role, but several studies have described a normal or low pressure at the cricopharyngeus. • “Achalasia” of the cricopharyngeus • UES does relax during swallow in Zenker’s patients • Dyscoordination of cricopharyngeal function
Clinical Presentation Most patients develop symptoms due to obstruction and retention • Upper esophageal dysphagia • Regurgitation • Aspiration • Halitosis • Voice change • Weight loss
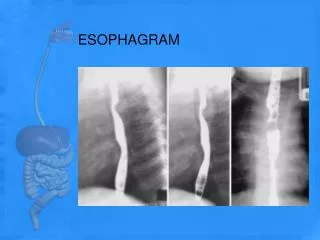
Diagnosis of Zenker’s Diverticulum • Barium swallow • Manometry if symptoms of reflux • Endoscopy
Diagnosis of Zenker’s Diverticulum • Endoscopy • laryngoscopy • short rigid esophagoscopy • flexible endoscopy • High aspiration risk • Keep patients sitting up • Rapid sequence intubations • Rigid suction at hand • Refractory to Selleck’s maneuver
Treatment options: open procedures • Diverticulectomy with myotomy • best for the large diverticulum • carries risks associated with esophageal repair • Diverticulopexy with myotomy • may be suitable for smaller (<2cm) diverticula • Myotomy alone • may prevent progression of mild symptoms associated with a small diverticulum
Treatment options: open procedures • Diverticulectomy or diverticulopexy without myotomy • not recommended • fails to address the basic functional abnormality
Diverticulectomy Mayo Clinic Series (n=888) • Morbidity=3% Mortality=1.2% • Recurrence=3.6% • Good or Excellent relief of dysphagia=93%
Diverticulopexy • May be useful if healing of a suture or staple line is a concern • Diverticulum is sutured to the prevertebral facia allowing dependent drainage • Sutures through the diverticulum (5-0 wire) can obliterate the lumen
Treatment options: endoscopic diverticulectomy • Described by Dohlman (1964) • Septum between the diverticulum and the esophagus is divided • 92-98% success rate at palliating dysphagia • 3% conversion rate to open procedure • 30% of cases endoscopic repair not attempted
Endoscopic Options Moscher 1917 Divided septum with a knife (punch biopsy) 7 patients- Abandoned following postoperative death Dohlman and Mattsson 1960 100 patients/fixed laryngoscope (better visualization) Endoscopic division of the common wall using a diathermy knife Symptom recurrence rate 7%, no significant complications were observed Mosher HP. Webs and pouches of the esophagus: their diagnosis and treatment. Surg Gynecol Obstet 25: 1917. 175–187 Dohlman G, Mattsson O. The endoscopic operation for hypopharyngeal diverticula. Arch Otolaryngol 71: 1960. 744–752
Endoscopic Options Van Overbeek 1982 12 patients (as compared to electrocoagulation) Septum divided with CO2 laser Several sessions with larger diverticula Operating microscope Collard 1993 30mm Endo-GIA stapler/eventually modified stapler tip Video assistance 6 patients- dysphagia relieved in 5 and improved in 1 van Overbeek JJ, Hoeksema PE, Edens ET.Microendoscopic surgery of the hypopharyngeal diverticulum using electrocoagulation or carbon dioxide laser. Ann Otol Rhinol Laryngol. 1984 Jan-Feb;93(1 Pt 1):34-6 Collard JM, Otte JB, Kestens PJ.Endoscopic stapling technique of esophagodiverticulostomy for Zenker's diverticulum. Ann Thorac Surg. 1993 Sep;56(3):573-6
OperativeConsiderations Diverticulum >3 cm in size Limitations to mouth opening Prominent overbite Cervical osteoarthritis/poor neck flexion
Transoral Stapling (TOS)- Technique Supine General anesthesia
Transoral Stapling - Technique EGD with placement of guidewire
Transoral Stapling - Technique Weerda diverticuloscope/laryngoscope (Karl Storz)
Transoral Stapling - Technique Stapler: Endo-GIA 30 (modified)
Transoral Stapling - Technique 5mm 30 degree thoracoscope
Transoral Stapling - Technique Autosuture Endostitch
Transoral Stapling - Technique Autosuture Endostitch
Comparative Studies • UPMC 2007 • Dysphagia scores comparable preoperatively (2.78 OS / 2.79 TOS ) • Improved significantly in both groups (1.1 TOS / 1.0 OS) • Follow up 17 months
Transoral Stapling of Zenker’s Diverticulum • Transoral treatment employed from beginning of century • Relative advantages • No incision/OR time/No pain/Short LOS/Earlier POs/ • Procedure of choice for recurrent Zenker’s diverticulum? • Procedure of choice with previous neck surgery?
Transoral Stapling of Zenker’s Diverticulum • Requires general anesthesia • Small diverticulum – contraindication • Introduction of scope/stapler limited in some patients • Residual spur • Individualized approach
Conclusions • The presence of a Zenker’s diverticulum is an indication for surgery • Symptoms frequently progress • Routine use of myotomy favored • Management of diverticulum after myotomy depends on size of residual pouch and patients condition • Rare contraindications to surgery
FEATURES Least common esophageal diverticulum Occurs within 10cm from the EG jxn and almost always of pulsion type Acquired diverticulum later in adult life Prevalence difficult to quantitate Asymptomatic patients not discovered Majority of patients have some form of esophageal dysmotility with functional esophageal obstruction
PATHOPHYSIOLOGY Increase intraluminal pressure against a relative obstruction causes mucosal herniation false diverticulum Altorki, Orringer, DeMeester suggest all patients have esophageal dysmotility Some association with: Achalasia Diffuse esohageal spasm Connective tissue diseases Hypertensive LES Reflux strictures
ASSOCIATED ESOPHAGEAL DISORDERS Nehra 2002 Castrucci 1998 51 27 5 6 12 26 6 4
SIGNS AND SYMPTOMS Dysphagia Regurgitation Halitosis Chest, epigastric pain Cough, hoarseness Aspiration pneumonia No correlation between size and severity of symptoms
PREOPERATIVE EVALUATION Barium esophagram Esophagoscopy to rule out achalasia or neoplasm Esophageal manometry Endoscopic placement *24hr ambulatory study increased diagnostic yield 24hr pH probe if GERD suspected *Nehra D, DeMeester TR et al., Ann Surg, 2002.
CONTROVERSY Should asymptomatic patients undergo repair? Does diverticulum size matter? Length of esophagomyotomy ? Anti-reflux procedure
TREATMENT Symptom severity Minimal conservative management Altorki recommends Rx in all patients Moderate to Severe surgical repair Left transpleural approach most common Diverticulectomy Long myotomy over 50-54 bougie Antireflux procedure controversial Minimally invasive approach Thoracoscopy Laparoscopy found similar to open
TRANSPLEURAL APPROACH • Left thoracotomy • Diverticulectomy • Long myotomy • Opposite the diverticulum • Including the length of the motor abnormality • ± Anti-reflux procedure • Incomplete Fundoplication • Dor, anterior 180° • Toupet, posterior 270° • Belsy thoracic, posterior 240°
DIVERTICULECTOMY Rotation and isolation of diverticulum
MYOTOMY Closure of muscularis propria over diverticulectomy
Myotomy carried onto the stomach 1-2 cm Antireflux procedure?
LONG MYOTOMY Including the length of the motor abnormality
TREATMENT Mayo Clinic Series 16yr Retrospective study - 112 Patients 71 pts. no symptoms 35 followed long term with no sequelae @ 7yrs 41 pts. symptomatic 33 underwent repair 90% dysphagia, 82% regurg, 30% aspiration 50% hiatal hernia 9% mortality 33% major complication (18% leak rate) Fair or poor long term function in 24% Benacci JC et al., Ann Thor Surg, 1993.
CORNELL EXPERIENCENEW YORK HOSPITAL 21 Patients Size 3-10cm 17/21 (81%) Transthoracic diverticulectomy with esophageal myotomy and anti-reflux procedure 24% pulmonary symptoms 52% dysphagia and regurgitation 43% achalasia All had abnormal esophageal motility 26% pulmonary complications Altorki NK, Skinner DB, J Thorac Cardiovasc Surg, 1993.
REVIEW OF SURGICAL SERIES D = diverticulectomy, M = myotomy, A = antireflux, DMA = combined treatment
MINIMALLY INVASIVE APPROACH Many small series ( leak rate) Found feasible and safe* Laparoscopic transhiatal approach and thoracoscopic approach Diverticulum divided with linear stapler Myotomy on opposite esophageal side Anti-reflux procedure Potential difficulty with a long myotomy via laparoscopic approach *Rosati R, et al. Laparoscopic treatment of epiphrenic diverticula. J Laparoendosc Adv Surg TechA. 2001 Dec;11(6):371-5
ASYMPTOMATIC PATIENTS Over a 12 yr period, enlargement was noted in 16%, significance unclear* High risk of aspiration found in 46%# Overall < 10% will develop sx’s Regular clinical and radiologic review once identified *Bruggeman LL, Seaman WB. Epiphrenic diverticula. An analysis of 80 cases. Am J Roentgenol Radium Ther Nucl Med, 1973; 119:266-276. #Altorki NK, Skinner DB, J Thorac Cardiovasc Surg, 1993.
CONCLUSIONS Epiphrenic diverticulae are always associated with esophageal motor disorders Symptomatic diverticulae should be repaired Operative repair in asymptomatic patients controversial Food or contrast retention potential indication Castrucci Series complications occur in 45% pts. Altorki, DeMeester Diverticulectomy, diverticulopexy, long myotomy yield a good result in 90% of pts. Anti-reflux repair as part of management prevails in more recent series (partial fundoplication, loose Nissen)