Download
1 / 40
460 likes | 719 Views
COLORECTAL POLYPS AND COLORECTAL CARCINOMA. COLONIC POLYPS. May occur in any part of the colon Majority of them arise in the rectum and sigmoid colon They tend to cause rectal bleeding (visible or occult) and may undergo malignant change

E N D
COLONIC POLYPS • May occur in any part of the colon • Majority of them arise in the rectum and sigmoid colon • They tend to cause rectal bleeding (visible or occult) and may undergo malignant change • If rectal polyps are found, the entire colon must be investigated- total colonoscopy • The larger the lesion the more likely it is to be malignant
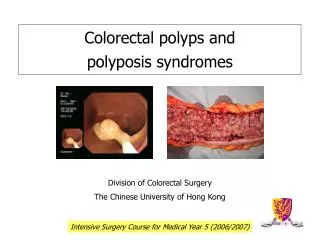
COLORECTAL POLYPS • Histopathologically- three patterns of growth: • tubular adenomas • villous adenomas • tubulo-villous adenomas
PHYSICAL EXAMINATION • General examination- features suggesting malignant disease: • Obvious weight loss • Palor of the skin • Abdominal distention • Hepatomegaly • Abdominal mass
PHYSICAL EXAMINATION • Rectal examination: • Finger can reach lesions as far as the its length 7-9 cm • Palpable fixed mass in Douglas pouch-sigmoid tumor dropped retrorectally • The glove inspected for blood and mucus
Risk Factors Risk increases with age • Nearly 90% of colon cancer patients • are over the age of 50. • Other risk factors include: • family or personal history of colon cancer • or polyps • chronic inflammatory bowel disease • hereditary colorectal syndromes • use of cigarettes and other tobacco products • high-fat/low fiber diet • physical inactivity
Symptoms Early colon cancer usually has no symptoms • Signs and symptoms typically occur only in advanced colon cancer. Symptoms may include: • Change in bowel habits lasting more • than a few days • Bleeding from the rectum • Blood in the stool • Cramping or gnawing stomach pains • Weakness and fatigue • Jaundice (yellow-green color of the skin & white part of the eye)
Colon Cancer Tests Fecal occult blood testing (FOBT) Barium enema Flexible sigmoidoscopy Colonoscopy Virtual Colonoscopy Get the test. Get the polyp. Get the cure.
Colonoscopy Advantages Detects >90% polyps and cancer Provides diagnosis and therapy Medicare covers average-risk Limitations Risks Availability Cost Compliance Get the polyp. Get the cure.
Are people getting tested? Testing rates remain far too low Fewer than half of Americans over age 50 report having had a recent colorectal cancer screening test Because of low testing rates, only 39% of colorectal cancers are detected at the earliest, most treatable stage
Ethnic/Racial differences Percentage who have never had screening colonoscopy Hispanics - 67% Black - 55.8% White, non-Hispanic – 47% Never married 60% Education less than high school diploma 58% vs 52% completed high school vs 46% with some college education 2005 data, AHRQ
Virtual Colonoscopy Spiral CT to generate 3D images Cleaning of bowel, distension with air Non invasive, no complications Notendorsed for CRC screening
Limitations Virtual Colonoscopy Variable results No screening studies No longitudinal studies Cost Does not allow for therapy
Stool DNA Now recommended by ACS and USMSTF for average risk individuals Multi-target DNA stool assay required to achieve adequate sensitivity and detect the various gene mutations 21 separate point mutations P53 DIA APC K-ras BAT-26
Video Capsule Colonoscopy In the process of development Battery life No clinical data available Anticipate to see clinical trials
Average Risk Individuals • No Symptoms • Age 50 • No risk factors
Current RecommendationsAverage Risk *Preferred strategy by ACG
Approach to Colon Cancer Testing Age < 50 yr Age 50 yr No family Hx NO family Hx No Screening Average Screening HNPCC or FAP 2 or more first-degree or 1 first-degree < 60 yrs 1 first-degree 60 yrs Genetic Counseling Colonoscopy every 5 yrs, starting age 40 Average-risk screening, starting age 40 Asymptomatic Men and Women YES family Hx
The flat polyp Techniques to improve detection Narrow-band imaging Chromoendoscopy Endocytoscopy Soitenko et al. JAMA March 2008
FAMILIAL POLIPOSIS COLI It is a rare autosomal dominant disorder Multiple colorectal polyps Rectal bleeding/ change in bowel habit The treatment- colorectal removal with ileoanal anastomosis, or panproctocolectomy with definitive ileostomy
Peutz-Jeghers syndrome It is an autosomal dominant inherited disorder characterized by intestinal hamartomatous polyps in association with mucocutaneous melanocytic macules. Patients with Peutz-Jeghers syndrome (PJS) have a 15-fold increased risk of developing intestinal cancer compared with that of the general population. Such cancer locations includes gastrointestinal and extraintestinal sites.