Download
1 / 30
300 likes | 315 Views
RBH Obesity Pathway. Theingi Aung & Greg Jones RBH 23 rd September 2015. Prevalence of Obesity. WHO; Obesity and overweight: fact sheet 311. Increasing at a epidemic rate globally 2.3 billions adults-overweight 700 millions-clinically obese Expected to rise further.

E N D
RBH Obesity Pathway TheingiAung & Greg Jones RBH 23rd September 2015
Prevalence of Obesity WHO; Obesity and overweight: fact sheet 311 Increasing at a epidemic rate globally 2.3 billions adults-overweight 700 millions-clinically obese Expected to rise further
Prevalence of obesity among adults aged 16+ years Health Survey for England 1993-2012 (3-year average)
Prevalence of Obesity • West Berkshire • BMI >50 N= 922 • BMI 40-50 N= 3559 • BMI 30-40 N= 2685
Moderately increased Increased Greatly increased (relative risk 2-3) (relative risk 1-2) (relative risk >>5) Relative risk of health problems associated with obesity Cancer (postmenopausal breast cancer, endometrial Coronary heart disease Diabetes Osteoarthritis (knees) Gall bladder disease cancer, colon cancer, prostate cancer, oesophageal cancer) Hyperuricaemia and Hypertension gout Dyslipidaemia Gastro-oesophageal reflux disease Low back pain Sleep apnoea Polycystic ovary Breathlessness syndrome Nonalcoholic fatty liver disease Impaired fertility Obstetric complications Increased anaesthetic risk
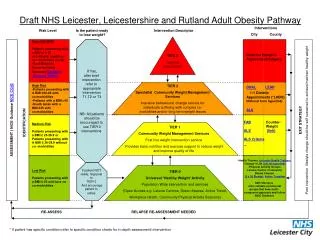
Models of care Tier 4 - Specialised Complex Obesity Services (including bariatric surgery) Tier 3 - MDT obesity service to provide an intensive level of input to patients. Tier 2 - Primary Care with Community Interventions Tier 1 - Primary Care and Community Advice
Tier 3/4 Specialist Complex Obesity Service at RBH Eligibility criteria Referral MDT assessment and optimisation of medical conditions before surgery Pre-op preparation programme & review Surgical MDT Pre-op clinic Surgery Post surgical care pathway
Clinical Commissioning Policy: Complex and Specialised Obesity Surgery (Tier 4) BMI > 40kg/m2 BMI >35 kg/m2 in the presence of other significant diseases Age <65 yr There must be formalised MDT led processes for the screening of co-morbidities the detection of other significant diseases The medical evaluation is mandatory prior to entering a surgical pathway. Morbid/severe obesity has been present for at least five years.
Bariatric surgery for recent onset type 2 diabetes • Consider Bariatric surgery with: • expedited assessment for BMI 35+ and recent onset T2DM. • with a BMI of 30-34.9 with recent onset T2DM • Lower BMI in Asian population with recent onset T2DM • as long as they are receiving or will receive assessment in tier 3 service.
Mode of referral • Choose & Book (medical team not surgical) • Letter direct to bariatric team • Referrals from other specialities
Time line of assessment of RBH Obesity pathway for surgery RBH Care pathway is available only for patients who want bariatric procedure; no medical pathway is currently not available: Exception: for BMI>50: minimum period of assessment 6 months.
Surgical MDT • Discuss difficult cases and see pre-op patients • Includes: • Consultant Bariatric Surgeon (3) • Metabolic Physician/Endocrinologist (1) • Consultant Bariatric Anaesthetist (2) • Specialist Dietician (2) • Bariatric Nurse Specialist (1) • Clinical Psychologist with Bariatric interest (2) • Specialist Nurse in Endocrine and Bariatric (1) • Surgical Pharmacist with Bariatric Interest (1) • Consultant Radiologist with Gastrointestinal and Bariatric interest (1)
Pre-op Discussion (Nice CG 189) • Potential benefits • Longer-term implications for surgery • Associated risks • Complications • Peri-operative mortality • Consent process in clinic All patients re-discussed at end of clinic and confirmation of surgery agreed
Surgical procedures at RBH • Laparoscopic Adjustable Gastric band • Laparoscopic Sleeve gastrectomy • Laparoscopic Roux-en-y gastric bypass • Gastric balloon • Revisional Bariatric surgery
Sleeve Gastrectomy Ghrelin GLP-1 PYY
Post-op care • In hospital: • Day of operation – water • Day 1 – free fluids • Day 2 – discharged home • Daily consultant review • Due to start an Enhanced recovery programme • On discharge: • All – Multivitamins, LMW heparin (2 week) • Sleeve/bypass • Ferrous fumerate • Calcit D3 • Vitamin B12 • Lansoprazole fast tab (3 months)
Follow-up (Nice CG 189) • Minimum 2 years within the bariatric service, including: • Monitoring nutritional intake and deficiencies • Monitoring co-morbidities • Medication review • Dietary and nutritional assessment • Physical activity advice and support • Psychological support tailored to the individual • Peer support • After discharge from bariatric service: • Annual monitoring of nutritional status and appropriate supplementation • Shared care model of chronic disease
Gastric band follow up • Surgical Clinic • 4 weeks • 4 months • Radiology- first band fill • 6-8 weeks • Specialist Nurse for band adjustment • 12 weeks • monthly until correct fill • 3 months • 6months • Specialist Nurse short notice/rescue clinic
Bypass/sleeve follow up • Surgical clinic: • 4 weeks • 4 months • 12 months • Rescue appointments if needed • Dietician: • 3 monthly in first year • 6 monthly until 2 years Drop in sessions for post-op: monthly at Diabetes centre)
Blood tests • To be performed at patients General Practice • Results to be acted upon by bariatric unit • Band • FBC, U& E, LFT annually • Bypass/Sleeve • FBC, U&E, LFT, Ferritin, Folate, Calcium, Vitamin D, PTH, • 3, 6, 12 months in first year and then annually • Vitamin B12 • 6, 12 months and then annually • Zinc, copper • Annually
Micronutrient replacement • All patients to buy • Complete A-Z multi-vitamin and mineral • GP to prescribe for sleeve and bypass patients • Calcium and Vit D Combined (Calcit D3) • daily for life • Vitamin B12 injection • 3 monthly • Iron Supplement (Ferrous Fumarate) • Daily for life
Time line of assessment of RBH Obesity pathway for surgery RBH Care pathway is available only for patients who want bariatric procedure; no medical pathway is currently not available: Exception: for BMI>50: minimum period of assessment 6 months.