Download
1 / 1

E N D
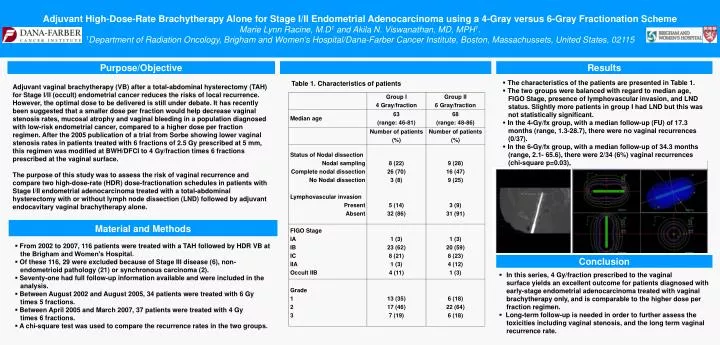
Adjuvant High-Dose-Rate Brachytherapy Alone for Stage I/II Endometrial Adenocarcinoma using a 4-Gray versus 6-Gray Fractionation SchemeMarie Lynn Racine, M.D1 and Akila N. Viswanathan, MD, MPH1. 1Department of Radiation Oncology, Brigham and Women's Hospital/Dana-Farber Cancer Institute, Boston, Massachussets, United States, 02115 Material and Methods Purpose/Objective Results • The characteristics of the patients are presented in Table 1. • The two groups were balanced with regard to median age, FIGO Stage, presence of lymphovascular invasion, and LND status. Slightly more patients in group I had LND but this was not statistically significant. • In the 4-Gy/fx group, with a median follow-up (FU) of 17.3 months (range, 1.3-28.7), there were no vaginal recurrences (0/37). • In the 6-Gy/fx group, with a median follow-up of 34.3 months (range, 2.1- 65.6), there were 2/34 (6%) vaginal recurrences (chi-square p=0.03), diagnosed 3 and 4 months after treatment. Table 1. Characteristics of patients Adjuvant vaginal brachytherapy (VB) after a total-abdominal hysterectomy (TAH) for Stage I/II (occult) endometrial cancer reduces the risks of local recurrence. However, the optimal dose to be delivered is still under debate. It has recently been suggested that a smaller dose per fraction would help decrease vaginal stenosis rates, mucosal atrophy and vaginal bleeding in a population diagnosed with low-risk endometrial cancer, compared to a higher dose per fraction regimen. After the 2005 publication of a trial from Sorbe showing lower vaginal stenosis rates in patients treated with 6 fractions of 2.5 Gy prescribed at 5 mm, this regimen was modified at BWH/DFCI to 4 Gy/fraction times 6 fractions prescribed at the vaginal surface. The purpose of this study was to assess the risk of vaginal recurrence and compare two high-dose-rate (HDR) dose-fractionation schedules in patients with Stage I/II endometrial adenocarcinoma treated with a total-abdominal hysterectomy with or without lymph node dissection (LND) followed by adjuvant endocavitary vaginal brachytherapy alone. • From 2002 to 2007, 116 patients were treated with a TAH followed by HDR VB at the Brigham and Women’s Hospital. • Of these 116, 29 were excluded because of Stage III disease (6), non- endometrioid pathology (21) or synchronous carcinoma (2). • Seventy-one had full follow-up information available and were included in the analysis. • Between August 2002 and August 2005, 34 patients were treated with 6 Gy times 5 fractions. • Between April 2005 and March 2007, 37patients were treated with 4 Gy times 6 fractions. • A chi-square test was used to compare the recurrence rates in the two groups. Conclusion • In this series, 4 Gy/fraction prescribed to the vaginal surface yields an excellent outcome for patients diagnosed with early-stage endometrial adenocarcinoma treated with vaginal brachytherapy only, and is comparable to the higher dose per fraction regimen. • Long-term follow-up is needed in order to further assess the toxicities including vaginal stenosis, and the long term vaginal recurrence rate. g