Download
1 / 1
10 likes | 206 Views
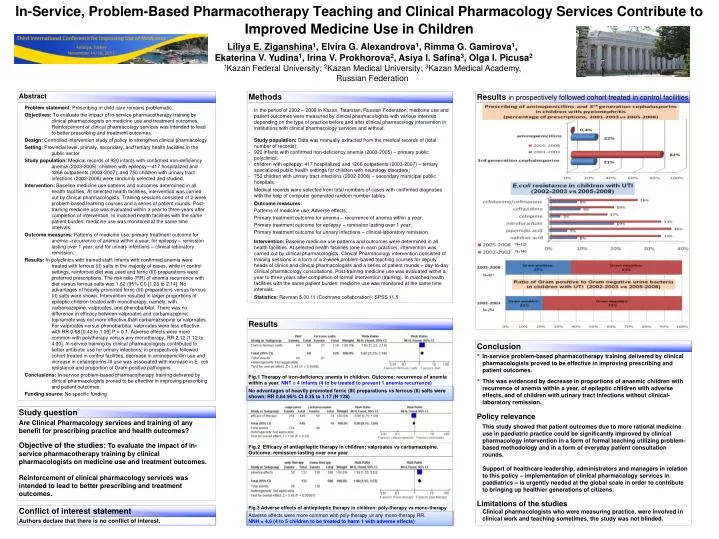
Problem statement : Prescribing in child care remains problematic.

E N D
Problem statement: Prescribing in child care remains problematic. Objectives: To evaluate the impact of in-service pharmacotherapy training by clinical pharmacologists on medicine use and treatment outcomes. Reinforcement of clinical pharmacology services was intended to lead to better prescribing and treatment outcomes. Design: Controlled intervention study of policy to strengthen clinical pharmacology Setting: Provincial level, primary, secondary, and tertiary health facilities in the public sector Study population: Medical records of 920 infants with confirmed iron-deficiency anemia (2003-2005); children with epilepsy—417 hospitalized and 1266 outpatients (2003-2007); and 750 children with urinary tract infections (2002-2008) were randomly selected and studied. Intervention: Baseline medicine use patterns and outcomes determined in all health facilities. At selected health facilities, intervention was carried out by clinical pharmacologists. Training sessions consisted of 2-week problem-based learning courses and a series of patient rounds. Post-training medicine use was evaluated within a year to three years after completion of intervention. In matched health facilities with the same patient burden, medicine use was monitored at the same time intervals. Outcome measures: Patterns of medicine use; primary treatment outcome for anemia –recurrence of anemia within a year; for epilepsy – remission lasting over 1 year; and for urinary infections – clinical-laboratory remission. Results: In polyclinics with trained staff, infants with confirmed anemia were treated with ferrous (II) salts in the majority of cases, while in control settings, reinforced diet was used and ferric (III) preparations were preferred prescriptions. The risk ratio (RR) of anemia recurrence with diet versus ferrous salts was 1.62 (95% CI) [1.23 to 2.14]. No advantages of heavily promoted ferric (III) preparations versus ferrous (II) salts were shown. Intervention resulted in larger proportions of epileptic children treated with monotherapy, namely, with carbamazepine, valproates, and phenobarbital. There was no difference in efficacy between valproates and carbamazepine; topiramate was not more effective than carbamazsepine or valproates. For valproates versus phenobarbital, valproates were less effective with RR 0.68 [0.42 to 1.09] P = 0.1. Adverse effects were more common with polytherapy versus any monotherapy, RR 2.12 [1.12 to 4.00]. In-service training by clinical pharmacologists contributed to better antibiotic use for urinary infections; in prospectively followed cohort treated in control facilities, decrease in aminopenicillin use and increase in cefalosporins-III use was associated with increase in E. coli resistance and proportion of Gram-positive pathogens. Conclusions: In-service problem-based pharmacotherapy training delivered by clinical pharmacologists proved to be effective in improving prescribing and patient outcomes. Funding source: No specific funding In-Service, Problem-Based Pharmacotherapy Teaching and Clinical Pharmacology Services Contribute to Improved Medicine Use in Children Liliya E. Ziganshina1, Elvira G. Alexandrova1, Rimma G. Gamirova1, Ekaterina V. Yudina1, Irina V. Prokhorova2, Asiya I. Safina3, Olga I. Picusa2 1Kazan Federal University; 2Kazan Medical University; 3Kazan Medical Academy, Russian Federation Abstract Methods Resultsin prospectively followed cohort treated in control facilities • In the period of 2002 – 2008 in Kazan, Tatarstan, Russian Federation, medicine use and patient outcomes were measured by clinical pharmacologists withvarious intervals depending on the type of practice before and after clinical pharmacology intervention in institutions with clinical pharmacology services and without. • Study population: Data was manually extracted from the medical records of (total number of records): • 920 infants with confirmed iron-deficiency anemia (2003-2005) – primary public polyclinics; • children with epilepsy: 417 hospitalized and 1266 outpatients (2003-2007) – tertiary specialized public health settings for children with neurology disorders; • 750 children with urinary tract infections (2002-2008) – secondary municipal public hospitals. • Medical records were selected from total numbers of cases with confirmed diagnoses with the help of computer generated random number tables. • Outcome measures: • Patterns of medicine use; Adverse effects; • Рrimary treatment outcome for anemia – recurrence of anemia within a year; • Primary treatment outcome for epilepsy – remission lasting over 1 year; • Primary treatment outcome for urinary infections – clinical-laboratory remission. • Intervention: Baseline medicine use patterns and outcomes were determined in all health facilities. At selected health facilities (one in each practice), intervention was carried out by clinical pharmacologists. Clinical Pharmacology intervention consisted of training sessions in a form of a2-week problem-based teaching courses for deputy heads of clinics and clinical pharmacologists and a series of patient rounds – day-to-day clinical pharmacology consultations. Post-training medicine use was evaluated within a year to three years after completion of formal intervention (training). In matched health facilities with the same patient burden, medicine use was monitored at the same time intervals. • Statistics: Revman 5.00.11 (Cochrane collaboration); SPSS 11.5. N=129 N=146 N=401 N=254 Results Conclusion • In-service problem-based pharmacotherapy training delivered by clinical pharmacologists proved to be effective in improving prescribing and patient outcomes. • This was evidenced by decrease in proportions of anaemic childrenwith recurrence of anemia within a year, of epileptic children with adverse effects, and of children with urinary tract infections without clinical-laboratory remission. • Policy relevance • This study showed that patient outcomes due to more rational medicine use in paediatric practice could be significantly improved by clinical pharmacology intervention in a form of formal teaching utilizing problem-based methodology and in a form of everyday patient consultation rounds. • Support of healthcare leadership, administrators and managers in relation to this policy – implementation of clinical pharmacology services in paediatrics – is urgently needed at the global scale in order to contribute to bringing up healthier generations of citizens. • Limitations of the studies • Clinical pharmacologists who were measuring practice, were involved in clinical work and teaching sometimes, the study was not blinded. Fig.1 Therapy of iron-deficiency anemia in children. Outcome: recurrenceof anemia within a year. NNT = 4 infants (4 to be treated to prevent 1 anemia recurrence) No advantages of heavily promoted ferric (III) preparations vs ferrous (II) salts were shown: RR 0.64 95% CI 0.35 to 1.17 (N 128) Study question Are Clinical Pharmacology services and training of any benefit for prescribing practice and health outcomes? Objective of the studies: To evaluate the impact of in-service pharmacotherapy training by clinical pharmacologists on medicine use and treatment outcomes. Reinforcement of clinical pharmacology services was intended to lead to better prescribing and treatment outcomes. Fig.2 Efficacy of antiepileptic therapy in children:valproates vs carbamazepine. Outcome: remission lasting over one year Fig.3 Adverse effects of antiepileptic therapy in children: poly-therapy vs mono-therapy Conflict of interest statement Adverse effects were more common with poly-therapy vs any mono-therapyRR. NNH = 4.6 (4 to 5 children to be treated to harm 1 with adverse effects) Authors declare that there is no conflict of interest.