Download
1 / 22
240 likes | 1.09k Views
IBS In The Elderly. Monica J. Cox ARNP-BC, MSN, MPH Geriatric Nurse Practitioner G.I. Nurse Practitioner Borland-Groover Clinic Jacksonville, Florida. OBJECTIVES. Describe Age-Related Changes In The Digestive System Discuss The Neurophysiology of Irritable Bowel Syndrome

E N D
IBS In The Elderly Monica J. Cox ARNP-BC, MSN, MPH Geriatric Nurse Practitioner G.I. Nurse Practitioner Borland-Groover Clinic Jacksonville, Florida
OBJECTIVES • Describe Age-Related Changes In The Digestive System • Discuss The Neurophysiology of Irritable Bowel Syndrome • Describe The Current Approaches For Evaluating and Treating Elderly Patients With Irritable Bowel Syndrome
Alarm Symptoms Suggestive of Organic Disease • HISTORY • Weight loss < 10 lbs • Nocturnal symptoms • Initial onset at age > 50 yrs • Significant travel history • Arthritis/rashes • FAMILY HISTORY • Colon cancer • Inflammatory bowel disease • Celiac disease
Alarm Symptoms Suggestive of Organic Disease - continued • PHYSICAL FINDINGS • Fever • Oral ulcers • Palpable abdominal mass • Guaiac-positive stool • Other physical bleeding or obstruction • LABORATORY EVALUATION • Increased white blood cell count • Anemia • Abnormal chemistry • Increased thyroid-stimulating hormone • Elevated sedimentation rate or C-reactive protein
Types Of Neurons In The Small Intestinal Enteric Nervous System
Rome Criteria III • At least 3 months, with onset at least 6 months previously of recurrent abdominal pain or discomfort** associated with 2 or more of the following: • Improvement with defecation; and/or • Onset associated with a change in frequency of stool; and/or • Onset associated with a change in form (appearance) of stool **Discomfort means an uncomfortable sensation not described as pain.
“Functional” Sydromesoften due to “Dysmotility” • Functional bowel disorders: • Non-ulcer dyspepsia • Irritable bowel syndrome • Defined motility disorders: • GI neuromuscular syndromes • Myopathies vs. Neuropathies
Dysfunction of Different GI OrgansProduces Similar Symptoms • Gullett – Chest pain, belching, dysphagia, regurg • LES – Chest pain, pyrosis, belching, regurg • Stomach – Regurg, fullness, dyspepsia, bloating • Small bowel – Fullness, dyspepsia, discomfort, bloating, change in bowel habits • Colon – Fullness, discomfort, variable bowel habits • Thus, it is often necessary to test all organs
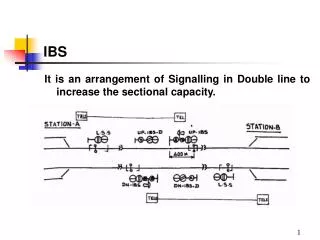
Too Slow Gas Fullness Bloating Cramps Altered Bowel Habits Too Rapid Gas Fullness Bloating Cramps Altered Bowel Habits Sx’s of Small Bowel DysmotilityMay Indicate Disordered Transit
Predominant Symptom Constipation: Infrequent bowel movements Obstructed defecation Diagnostic Tests Colonoscopy Whole-gut transit test Anorectal motility plus balloon expulsion Defecating proctography Diagnostic Evaluation
Predominant Symptom Diarrhea: Diagnostic Evaluation Diagnostic Tests • 24-hour stool volume and fat study • Stool osmolality, electrolytes, and laxatives • Transit test: small bowel and colon • Colonic biopsies • Breath test
Predominant Symptom Pain: Diagnostic Evaluation Diagnostic Tests • Plain abdominal x-ray • Small bowel follow-through examination • CT/MR imaging • Pelvic ultrasound