Download
1 / 34
340 likes | 831 Views
Modeling antibiotic resistance in populations: from deterministic to stochastic to agent-based models. . Laura TEMIME. G Thomas, PY Boëlle, D Guillemot L Opatowski, Y Pannet . Modeling antibiotic resistance in populations. Why model resistance?

E N D
Modeling antibiotic resistance in populations: from deterministic to stochastic to agent-based models. Laura TEMIME G Thomas, PY Boëlle, D Guillemot L Opatowski, Y Pannet
Modeling antibiotic resistance in populations Why model resistance? • To achieve better understanding of underlying processes in resistance selection • To predict future changes • To evaluate control measures such as: • Reduction of antibiotic consumption in the community • Hand washing, systematic isolation or use of rapid diagnostic tests in hospitals
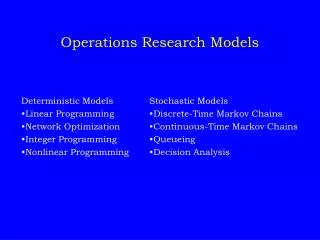
Different modeling approaches Available approaches for modeling antibiotic resistance selection in a population: • In large communities (e.g. country): • Compartmental deterministic models Good prediction of the average behavior • In smaller settings (e.g. schools, hospitals): • Compartmental stochastic models Information on the variability of processes • Agent-based models Data on the individual level
Presentation outline • Modeling pneumococcal resistance to penicillin using a compartmental model: • Deterministic model • Stochastic model Several papers between 2003 and 2006 • Modeling the selection and spread of antibiotic resistance in hospital settings: • Individual-based model Preliminary results, work in progress
I- Modeling the selection of pneumococcal resistance to penicillin in France A deterministic model (Temime L, Boëlle PY, Courvalin P, Guillemot D; Emerg Infect Dis, 2003)
Context overview • S. pneumoniae: • Human pathogen (otitis, pneumonia, meningitis) 3-5 million deaths / year worldwide • Frequent asymptomatic carriage Up to 40% carriers among children • Widespread antibiotic resistance In France over 60% of strains exhibit decreased sensitivity to penicillin frequently observed multiple resistance
A specific resistance mechanism S. pneumoniae resistance to penicillin: Progressive decrease of sensitivity (MIC)
A specific model • Objective = combining two levels for pneumococcal resistance selection: • Intra-individual evolution of strains reproducing the resistance mechanism • Inter-individual transmission of strains • Model characteristics: • Compartmental deterministic model (partial differential equations) • Progressive increase of resistance levels Colonized compartments structured by MIC (continuous)
A specific model: illustration Unexposed to antibiotics Exposed to antibiotics Genetic events progressive MIC increase
8 days 1 tmt / 2 yrs Model parameters 2.2 months
D(d) = (m) = Effects of antibiotic exposure • Colonization may persist with probability: • MIC may increase due to genetic events, according to the law:
Validation of model predictions Model predictions CNRP data (87-97) • 1987 : mostly antibiotic sensitive strains • 1997 : bimodal distribution of MICs
Applications of this deterministic model • Predictions for N. meningitidis: • Differences in resistance levels of pneumococci and meningococci can be explained by their natural histories of colonization alone • High resistance levels expected in years to come • Pneumococcal conjugate vaccination: • Short-term impact on carriage and resistance • BUT expected re-increase in resistance in the long-term, due to replacement of vaccine strains by non-vaccine strains which will become resistant (Temime L, Boëlle PY, Valleron AJ, Guillemot D; Epid Infect, 2005) (Temime L, Guillemot D, Boëlle PY; Antimicrob Agents Chemother, 2004)
II- Modeling the selection of pneumococcal resistance to penicillin A stochastic model (Temime L, Boëlle PY, Courvalin P, Guillemot D; Emerg Infect Dis, 2003) (Temime L, Boëlle PY, Thomas G; Math Pop Studies, 2005)
Motivation • Shortcomings of the deterministic model: • Averaged predictions • No information on variability • Identical predictions regardless of population size Developing a stochastic version of the model will allow: • More realism in the description • Better predictions in small populations • Information on the variability of predicted phenomena
General principles • Same compartmental model than in the deterministic setting • But transitions between compartments are considered random Associated transition probabilities For large population sizes, the deterministic solution approximates the mean stochastic epidemics
Results in a town-like community (1000 individuals) For a given MIC: Time before the first emergence of a strain with this MIC Time before 20% of strains will have reached this MIC Penicillin-resistant pneumococcal strains will emerge on average 20 years after the introduction of penicillin, but it may be 10-30 years.
III- Modeling the selection of S. aureus multi-resistance in hospital settings (ICUs) An agent-based model
Context overview • Staphylococcus aureus : • Human pathogen (skin infections, septicemia, endocarditis) • 10-40% asymptomatic carriers • Colonization duration?? • Antibiotic resistance : • Widespread penicillin resistance • Methicillin resistance (MRSA) common in hospital settings since the 1960’s (30-50% of all strains) • Emergence of MRSA in the community in recent years
Some important questions • What are the determinants for persistence of a staphylococcal strain in a hospital setting? • Why aren’t NO-MRSA successful outside hospitals? • Which context could allow for the successful introduction of CA-MRSA in hospitals? • What would be the consequences?
Why an agent-based model? • Individual-based or agent-based modeling has proved useful for: • Modeling epidemic spread in an urban network (Eubank et al., Nature, 2004) or even at a countrywide scale (Longini et al., Am J Epid, 2004) • Simulating healthcare activities in a hospital setting (Boelle et al., Comput Biom Res, 1998) • Modeling pathogen dissemination in an ICU (Hotchkiss et al., Crit Care Med, 2005) and interventions Allows for more realism and easier description of individual behaviors
Model structure: hospital ward (ICU) Patient 1 Patient 2 Patient 3 Patient 4 … Ward corridors / Staff room Doctors Nurses … … 1 2 3 4 1 2 3 4 ROOMS …
Model structure: agents and agent characteristics (2) Transmission of colonization through infectious contacts
First model outcomes (1) Real-time graphical display of the hospital ward: Follow-up of the geographical spread of micro-organisms
First model outcomes (2) Temporal changes in proportions of colonized individuals:
First model outcomes (3) Who colonized whom? History of transmission:
Perspectives for the ABM • Lots of possible uses: • Educational tool • Assessment of control measures taking into account individual behaviors (non compliance) • Predictions for dominance in a two strain-environment (CA-MRSA and NO-MRSA) • Disadvantages: • Not a mathematical model no analytical expression available • Costly in simulation time • Large amount of data needed
Need for data • Data for model building (parameter values): • Micro-organism characteristics (duration of colonization, invasivity, ...) • Human characteristics (daily activities and contacts, immunity status, ...) • Resistance characteristics (mechanism of emergence, current susceptibility levels, ...) • Data for model validation: • Historical data on emergence and spread of resistant strains in specific settings Allows comparison with model predictions
Specific needs for different kinds of models The amount of required data increases with model complexity: • Compartmental models: • Mean characteristics in the population: duration and frequency of antibiotic exposure, infectious contact rate • Mean characteristics of the micro-organism: duration of colonization, susceptibility to antibiotic exposure • Resistance mechanism characteristics • Agent-based models: • Similar characteristics at the individual level • Supplemental data on individual behaviors
Infectious contact rate • Complex parameter which includes: • The frequency of inter-human contacts • The transmissibility of the micro-organism • Estimation strategies: • Not directly observed in populations • Often calibrated to reflect observed colonization • May be estimated using MCMC methods from longitudinal data (Cauchemez et al., BMC Inf Dis, 2006) • Will be measured in hospital settings using “contact tracers” carried by staff and patients (MOSAR project, WP7)
Conclusions • Rising impact of the modeling approach to study antibiotic resistance selection over the last 15 years : • More published models • More cited by a wider audience • Recent developments: more complex models which require more complex data Antibiotic resistance modeling can only be satisfyingly achieved through a collaboration with microbiologists, physicians, etc.