Download
1 / 17
170 likes | 365 Views
Nocosomial infection with Vancomycin-dependent Enterococci. Michelle Nguyen Bioc 230 10/11/04. Preview. Cases Molecular profiling of VDE Case control study Discussion. Case 1. 32 y.o woman with h/o type 1 DM, ESRD Kidney-pancreas transplant

E N D
Nocosomial infection with Vancomycin-dependent Enterococci Michelle Nguyen Bioc 230 10/11/04
Preview • Cases • Molecular profiling of VDE • Case control study • Discussion
Case 1 • 32 y.o woman with h/o type 1 DM, ESRD • Kidney-pancreas transplant • Post-op infection with VR Enterococcus faeciumTx with antibiotics • Abdominal fluid culture VR E. faecium that cannot grow w/o Vancomycin • Refractory sepsisdeath (day 268)
Case #2 • 40 y.o woman with h/o type I DM, ESRD • Kidney-pancreas transplant • Post-op: VRE from intraabdominal culturesremove kidney and pancreas • Antibiotic tx with IV streptogramins • Refractory VREdeath
Case #3 • 47 y.o woman with h/o CML • Matched-unrelated donor bone marrow transplant • Post-op: severe GVHD, acute renal failure, bacteremia with Corynebacteriumvancomycin • UTI with VREnot eradicated • Death due to refractory GVHD with multiple organ failure (day 87)
Tip off: what are the common points • Nocosomial infections • Comorbidities: DM, kidney dysfunction,tranplants post-op complications • Bacteremia with VDE • Broad use of antibiotics and immunosuppressive drugs (what are the risks??)
Characterizing VDE • Criteria • VRE: growth in 6ug/ml Vancomycin, MIC>8ug/ml Vanco • VDE: cannot growth without 6ug/ml Vanco with multiple subcultures • Molecular profile • Susceptibility testing: Vanco disk, D-ala-D-ala disk • Resistance gene vanA and vanB: PCR • Strain relation (distinct clones?): Pulsed-field gel electrophoresis (PFGE) • Spontaneous reversion from VDE to VRE: serial dilutions of culture grown in Vanco+ broth to Vanco+/- agar plates
Susceptibility Test Result Revertant VDE
Molecular profile of VDE • Strain: E. faecium • Resistance gene: vanA (2), vanB (1) • Resistance profile: penicillins, gentamicin, erythromycin • Susceptibility: streptogramins, teicoplanin • Spontaneous reversion: around 1x10-6 except for strain 3 (2.6x10-3) • Growth not supported by D-ala-D-ala
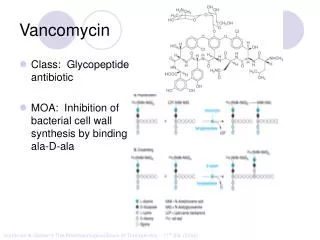
Proposed mechanism for Vancomycin dependence • Loss of D-ala-D-ala ligase in VRE strain • Vancomycin induces production of D-ala-D-lactate ligase • Require prolonged exposure to Vancomycin
Case control study • 3 patients with nocosomial VDE infection • 10 patients with nocosomial VRE infection • 10 at-risk patients not infected with enterococci • Matched by age and admission to same service
Specific findings • Length of exposure to antimicrobials • Vancomycin • 3rd generation cephalosporins • Mortality • Gender • Exposure to ICU
Possible risk factors • Intense use of 3rd generation cephalosporins • Renal insufficiency • Spontaneous reversionVanco discontinuation might not be sufficient to treat VDE infection.