Download
1 / 25
250 likes | 574 Views
PVD, AAA and renal stones. Dörthe and Jo. Case Study. Bob, 70 years old 1 month history intermittent back pain. HPC. PMH/ Risk factors. Presenting complaint of AAA. On Examination. Feel above the umbilicus for aortic aneurysm If leaking or rupture. Definition.

E N D
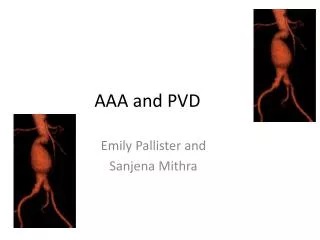
PVD, AAA and renalstones Dörthe and Jo
Case Study • Bob, 70 yearsold • 1 monthhistoryintermittent back pain
OnExamination • Feelabove the umbilicus for aorticaneurysm • If leakingorrupture
Definition • Abnormal dilatation of abdominal aorta over 2x the normal size (2cm) orenlargement over 3cm • Most commonlyaffectsinfrarenal aorta 95% withiliacinvolvement in 30% • 6000 deaths per year in england and wales
True or false aneurysm? • True aneurysm • Dilatation of all threelayers of vessel • False aneurysm • Dilatation of artery not involving all threelayers
Aetiology • Atherosclerotic in 95% • 5% inflammatory • Others • Traumatic • Infective (mycoticaneurysm) • CTD – Ehler’sDanlos,Marfans
Pathophysiology • Decrease of amount of medial and adventitialelastin • Otherpossibleplaces • Aorta • Iliac • Popliteal • Femoral arteries
Investigations • Acute – CT scan, Bloods, ECG • US for screening purposes ( over 65 ) • AAA on AXR – eggshellappearance due to calcificationaneurysmwall
Management • Conservative • If asymptomatic • Under 5.5cm • Regularfollow ups with US • Management of cardiovascularrisk factors • Surgical • Prostheticgraftplacement – rewrapping of nativeaneurysmaround to reduceincidence of enterograftfistula formation • Endovascular EVAR – placementstentthrough distant percutaneousaccess
Criteria for surgery • AAA over 5.5 cm • Rupture • Rapid growth • Embolisation of plaque • Symptomatic
Complications General Of surgery Electivemortality – under 4% Emergencysurgerymortality 50% Haemorrhage Graftinfection Thrombosis/embolism Colonicischaemia Renalfailure • Risk of rupture • Under 5cm – 4% • 5-7cm diameter – 7% • More than 7cm – 20% • Rupture • Distalembolus • Suddencompletethrombosis • Fistulae formation • Infection
Definition • Alsocalledperipheralarterialdisease • Occlusiveatheroscleroticdisease in lowerextremities • Occlusiondistal to aorticarch • Up to 12% of 55-70year oldaffected • Rare causes – vasculitis, Buerger’sdisease
Atherosclerosis • Atheromascontainingcholesterol and lipid form withinintima and inner media, oftenaccompanied by ulceration and smoothmusclehyperplasia • Risk factors – hypertension, smoking, diabetes, FHx, hypercholesterolaemia, high LDL, obesity
Onexamination • Legs • Weak/ absent pulses • Reduced CRT • Cold, pale legs • Hairloss • Atrophic skin changes • Painful, punched out ulcers – pressureareas • venousulceration – medialmalleolus • Alsoexamine CVS
Investigations • HandheldDoppler • ABPI • Normal= 1, claudication <0.6, rest pain <0.4 • Bloods–anaemia, ESR, thrombophilia screen, lipids • ECG - ?CAD • ArterialDuplex • CT angiogram • Angiogram
Cx of PVD • Amputation • Gangrene • Dry – drynecrosis of tissuewithoutsigns of infection • Wet – moistnecrotictissuewithsigns of infection • Ulcers • Risk of limblosswithclaudication 5% per year • Risk of limblosswith rest pain over 50% per year
SurgicalManagement • Indications • Disablingclaudication • Criticalischaemia • Weak/absent femoral pulses • Angioplasty +- stenting • Surgicalbypassgraft
Prognosis • Highrisk for all-riskmortality, especiallycardiovascular • 15% progress to criticalischaemia • 50% improve • 25% stabilise • 20% worsen • 20% need intervention • 8% need amputation