Download
1 / 1

E N D
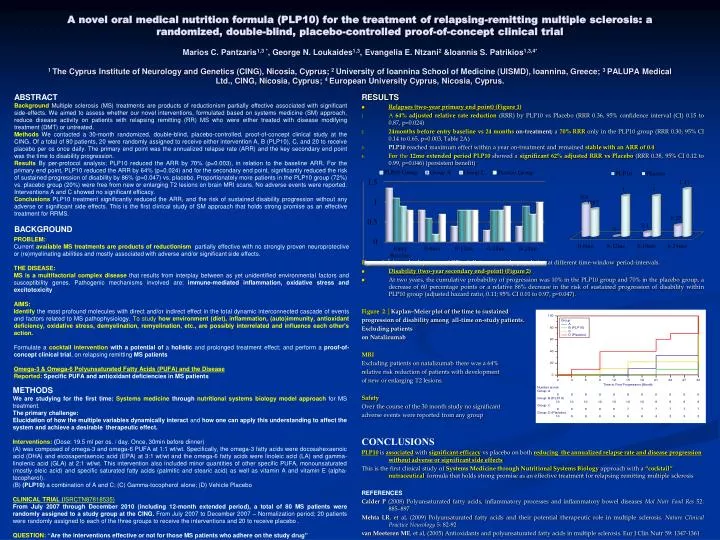
A novel oral medical nutrition formula (PLP10) for the treatment of relapsing-remitting multiple sclerosis: a randomized, double-blind, placebo-controlled proof-of-concept clinical trialMarios C. Pantzaris1,3 *, George N. Loukaides1,3, Evangelia E. Ntzani2 &Ioannis S. Patrikios1,3,4* 1 The Cyprus Institute of Neurology and Genetics (CING), Nicosia, Cyprus; 2 University of Ioannina School of Medicine (UISMD), Ioannina, Greece; 3 PALUPA Medical Ltd., CING, Nicosia, Cyprus; 4 European University Cyprus, Nicosia, Cyprus. ABSTRACT BackgroundMultiple sclerosis (MS) treatments are products of reductionism partially effective associated with significant side-effects. We aimed to assess whether our novel interventions, formulated based on systems medicine (SM) approach, reduce disease activity on patients with relapsing remitting (RR) MS who were either treated with disease modifying treatment (DMT) or untreated. MethodsWe contacted a 30-month randomized, double-blind, placebo-controlled, proof-of-concept clinical study at the CING. Of a total of 80 patients, 20 were randomly assigned to receive either intervention A, B (PLP10), C, and 20 to receive placebo per os once daily. The primary end point was the annualized relapse rate (ARR) and the key secondary end point was the time to disability progression. ResultsBy per-protocol analysis; PLP10 reduced the ARR by 70% (p=0.003), in relation to the baseline ARR. For the primary end point, PLP10 reduced the ARR by 64% (p=0.024) and for the secondary end point, significantly reduced the risk of sustained progression of disability by 86% (p=0.047) vs. placebo. Proportionately more patients in the PLP10 group (72%) vs. placebo group (20%) were free from new or enlarging T2 lesions on brain MRI scans. No adverse events were reported. Interventions A and C showed no significant efficacy. Conclusions PLP10 treatment significantly reduced the ARR, and the risk of sustained disability progression without any adverse or significant side effects. This is the first clinical study of SM approach that holds strong promise as an effective treatment for RRMS. BACKGROUND RESULTS • Relapses (two-year primary end point) (Figure 1) • A 64% adjusted relative rate reduction (RRR) by PLP10 vs Placebo (RRR 0.36, 95% confidence interval (CI) 0.15 to 0.87, p=0.024) • 24months before entry baseline vs 24 months on-treatment; a 70% RRR only in the PLP10 group (RRR 0.30; 95% CI 0.14 to 0.65, p=0.003, Table 2A) • PLP10 reached maximum effect within a year on-treatment and remained stable with an ARR of 0.4 • For the 12mo extended period PLP10 showed a significant 62% adjusted RRR vs Placebo (RRR 0.38, 95% CI 0.12 to 0.99, p=0.046) (persistent benefit) Figure 1.│Annual relapse rate (ARR) of all-time on-study population at different time-window period-intervals. • Disability (two-year secondary end-point) (Figure 2) • At two years, the cumulative probability of progression was 10% in the PLP10 group and 70% in the placebo group, a decrease of 60 percentage points or a relative 86% decrease in the risk of sustained progression of disability within PLP10 group (adjusted hazard ratio, 0.11; 95% CI 0.01 to 0.97, p=0.047). Figure 2.│Kaplan–Meier plot of the time to sustained progression of disability among all-time on-study patients. Excluding patients on Natalizumab MRI Excluding patients on natalizumab there was a 64% relative risk reduction of patients with development of new or enlarging T2 lesions. Safety Over the course of the 30 month study no significant adverse events were reported from any group CONCLUSIONS PLP10is associatedwith significant efficacyvs placebo on both reducing the annualized relapse rate and disease progression without adverse or significant side effects This is the first clinical study of Systems Medicine through Nutritional Systems Biology approach with a “cocktail” nutraceuticalformula that holds strong promise as an effective treatment for relapsing remitting multiple sclerosis REFERENCES Calder P (2008) Polyunsaturated fatty acids, inflammatory processes and inflammatory bowel diseases Mol Nutr Food Res 52: 885–897 Mehta LR, et al, (2009) Polyunsaturated fatty acids and their potential therapeutic role in multiple sclerosis. Nature Clinical Practice Neurology 5: 82-92 van Meeteren ME, et al, (2005) Antioxidants and polyunsaturated fatty acids in multiple sclerosis. Eur J ClinNutr 59: 1347-1361 PROBLEM: Current available MS treatments are products of reductionism, partially effective with no strongly proven neuroprotective or (re)myelinating abilities and mostly associated with adverse and/or significant side effects. THE DISEASE: MS is a multifactorial complex disease that results from interplay between as yet unidentified environmental factors and susceptibility genes. Pathogenic mechanisms involved are: immune-mediated inflammation, oxidative stress and excitotoxicity AIMS: Identifythe most profound molecules with direct and/or indirect effect in the total dynamic interconnected cascade of events and factors related to MS pathophysiology. To study how environment (diet), inflammation, (auto)immunity, antioxidant deficiency, oxidative stress, demyelination, remyelination,etc., are possibly interrelated and influence each other's action. Formulate a cocktail intervention with a potential of a holistic and prolonged treatment effect; and perform a proof-of-concept clinical trial, on relapsing remitting MS patients Omega-3 & Omega-6 Polyunsaturated Fatty Acids (PUFA) and the Disease Reported: Specific PUFA and antioxidant deficiencies in MS patients METHODS We are studying for the first time:Systems medicine throughnutritional systems biology model approach for MS treatment. The primary challenge: Elucidation of how the multiple variables dynamically interact and how one can apply this understanding to affect the system and achieve a desirable therapeutic effect. Interventions: (Dose: 19.5 ml per os. / day. Once, 30min before dinner) (A) was composed of omega-3 and omega-6 PUFA at 1:1 wt/wt. Specifically, the omega-3 fatty acids were docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) at 3:1 wt/wt and the omega-6 fatty acids were linoleic acid (LA) and gamma-linolenic acid (GLA) at 2:1 wt/wt. This intervention also included minor quantities of other specific PUFA, monounsaturated (mostly oleic acid) and specific saturated fatty acids (palmitic and stearic acid) as well as vitamin A and vitamin E (alpha-tocopherol). (B) (PLP10) a combination of A and C; (C) Gamma-tocopherol alone; (D) Vehicle Placebo CLINICAL TRIAL (ISRCTN87818535) From July 2007 through December 2010 (including 12-month extended period), a total of 80 MS patients were randomly assigned to a study group at the CING. From July 2007 to December 2007 – Normalization period; 20 patients were randomly assigned to each of the three groups to receive the interventions and 20 to receive placebo . QUESTION: “Are the interventions effective or not for those MS patients who adhere on the study drug”