Download
1 / 23
230 likes | 239 Views
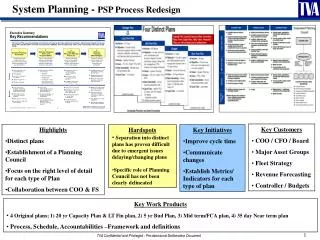
CDI Process Redesign. Meeting PSI Quality Review and Reporting Challenges. Shelia Bullock, BSN,.

E N D
CDI Process Redesign Meeting PSI Quality Review and Reporting Challenges
Shelia Bullock, BSN, Mrs. Bullock graduated with a Diploma in Nursing from Carraway Methodist Hospital School of Nursing and 2 years later from the University of North Alabama with her BSN. She earned her MBA from Belhaven University and is currently enrolled in the DHA program at UMMC. Shelia holds certifications in CDI, Coding and Case Management. Her nursing career spans over 30 years. She has worked as a staff nurse, in hospital nursing management, in commercial insurance as an auditor, implemented a case management and disease management program for a commercial insurance carrier, managed a hospital utilization review department and case management in a prison health system. Currently, she is the Associate Director of the Clinical Documentation Improvement Program at UMMC.
Disclosure Statement Speaker has no significant financial interest and this presentation does not have any commercial support. There is no investigational or unlabeled uses of a product in this presentation. The material is designed and provided to communicate information about clinical documentation, coding and compliance in an educational format and manner. The author is not providing or offering legal advice but, rather, practical and useful information and tools to achieve compliant results in the area of clinical documentation, data quality, and coding. Every reasonable effort has been taken to ensure that the educational content provided is accurate and useful. Applying best practice solutions, altering work flow, and achieving results will vary with each individual and clinical situation.
University of Mississippi Medical Center • Academic Medical Center 720 beds • Level I Trauma • Level 3C NICU • Children’s Hospital • Transplant Center • Heart, Kidney and Kidney Pancreas, Bone Marrow, Liver
Objectives • Discuss elements of Patient Safety Indicators (PSI) • Explain the importance of a PSI Review Process • Evaluate your hospital’s PSI Review Process
What are Patient Safety Indicators (PSIs)? • Set of measures developed at the national level by AHRQ (Agency for Healthcare Research and Quality) • Helps hospitals identify serious medical errors • Evidence reveals most PSIs are preventable
Why review? • These events are likely amenable to prevention by changes at the system or provider level. • PSIs and HACs are factored into quality of care ratings • Payment is impacted
Who uses? • CMS • Other Payers • Healthgrades • Leapfrog • Consumers • Others
What are the data sources? • CMS • Final paid inpatient claims • AHRQ • Healthcare Cost Utilization Program (HCUP) databases • State data • All payer population
PSIs List • PSI 02 Death Rate in Low-Mortality DRGs • PSI 03 Pressure Ulcer Rate • PSI 04 Death Rate Among Surgical Inpatients with Serious Treatable Conditions • PSI 05 Retained Surgical Item or Un-retrieved Device Fragment Count • PSI06 Iatrogenic Pneumothorax • PSI 07 Central Venous Catheter Related Blood Stream Infections • PSI 08 Postoperative Hip Fracture Rate • PSI 09 Perioperative Hemorrhage and Hematoma Rate • PSI 10 Postoperative Physiologic and Metabolic Derangement Rate • PSI 11 Postoperative Respiratory Failure • PSI 12 Perioperative Pulmonary Embolism or Deep Vein Thrombosis Rate • PSI 13 Postoperative Sepsis Rate • PSI 14 Postoperative Wound Dehiscence Rate • PSI 15 Accidental Puncture or Laceration
PSI Definitions • PSIs Measures: • By rate • By count • PSI Measure Characteristics: • Numerator cases (ex: pressure ulcer) • Denominator cases (patients at risk of having a pressure ulcer) • Factors that exclude a case from a denominator: • Admission Type • Diagnosis and Procedure Codes • Age • Others
PSI 90 • Compilation of 11 PSIs • PSIs 3, 6, 7, 8, 9, 10, 11, 12, 13, 14 & 15 • Based on observed to expected ratios • Most are surgical related
Why change the review process? • Number of PSIs increasing • Negative impact on public reporting • Record review revealed all reported PSIs were not actual PSIs • Documentation didn’t reflect a true picture • The concept of PSI was not totally understood by Coders, CDI nor providers • PSI were identified after billing, so if an error was found it was often to late to make corrections
Prior Process Concurrent Retrospective Focused on CMS Hospital Acquired Condition List Query Retrospectively Minimal MD review Data not transparent to providers WQ in EHR Partnership with Infection Prevention, Wound Care and Risk Management Weekly HAC Claims Report • Focused on CMS Hospital Acquired Condition List • Query Concurrently • Partnership with Infection Prevention, Wound Care and Risk Management
Process Redesign Concurrent Retrospective HACs and PSI 90 are a focus Expanded WQs in EHR RN Reviewer controls release of claims to billing MD review of all questionable and actual cases Data validated and reported monthly Intranet Scorecard • HACs and PSI 90 are a focus • Referral to Retrospective Review (flag to hold claim from final billing)
Official Coding Guidelines Documentation of Complications of Care: Code assignment is based on the provider’s documentation of the relationship between the condition and the care or procedure. The guideline extends to any complications of care, regardless of the chapter the code is located in. It is important to note that not all conditions that occur during or following medical care or surgery are classified as complications. There must be a cause-and effect relationship between the care provided and the condition, and an indication in the documentation that it is a complication. Query the provider for clarification, if the complication is not clearly documented. ICD-10-CM Section I. B. 16
How can PSI data be used to improve patient safety? • Review and synthesize the evidence based and best practices from scientific literature • Work with multiple disciplines and departments involved in care of patients to redesign care based on best practices with an emphasis on coordination and collaboration • Evaluate information technology solutions • Implement performance measurements for improvement and accountability
Challenges and Lessons Learned • Create a no blame culture • Erroneously high number of an adverse event misdirects quality and safety efforts and affects our public image and reimbursement • For majority of real AHRQ PSI cases, quality of care was excellent • Remaining proactive concerning updates to the AHRQ PSI technical specifications • Conversion of I-10 impact on PSIs