Download
1 / 30
300 likes | 441 Views
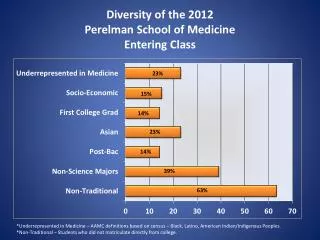
How often do immunomodulators and/or biologics cause lymphoma and/or cancer, and can we prevent lymphoma and/or cancer in our patients?. James D. Lewis, MD, MSCE Perelman School of Medicine University of Pennsylvania. There is never enough time to say everything that you want to say. Case.

E N D
How often do immunomodulators and/or biologics cause lymphoma and/or cancer, and can we prevent lymphoma and/or cancer in our patients? James D. Lewis, MD, MSCE Perelman School of Medicine University of Pennsylvania
There is never enough time to say everything that you want to say
Case • 35 y.o. male recently diagnosed with ileocolonic CD • Now steroid dependent • Treating physician recommends infliximab + azathioprine • Patient is concerned about risk of lymphoma
Questions • Does immunosuppressant therapy increase the risk of lymphoma? • Do the benefits outweigh the risks? • Is there anything I can do to decrease the risk of lymphoma?
AZA/6-MP & Lymphoma: Meta-analysis SIR = 4.06, 95% CI 2.01 – 7.28 Kandiel A et al. Gut. 2005:54:1121-25
CESAME - Lymphoma Beaugerie L. Lancet 2009 DOI:10.1016/S0140-6736(09)61302-7
Anti-TNF & Lymphoma: Meta-analysis Siegel C. ClinGastroenterolHepatol 2009;7:874-81 NHL rate – 6.1 per 10,000 p-y of exposure
Combination Therapy and Risk of Lymphoma • (1) BeaugerieL. Lancet 2009;374:1617-1625. (2) Herrinton L. Am J Gastroenterol 2011;106(12):2146-2153. (3) Khan N. Gastro 2013;145:1007-15(4) Osterman M. Gastro In press.
Clinical Questions • Does immunosuppressant therapy increase the risk of lymphoma? • Thiopurines – yes, but risk may revert after discontinuation • TNF – Possibly • Combination – More than TNF monotherapy, possibly more than thiopurinemonotherapy • Do the benefits outweigh the risks?
Number Needed to Harm ‡ Kandiel A et al. Gut. 2005:54:1121-25 * 5 year survival = 68% for NHL, 85% for HD, estimated at 75% for this example
Relationship of Age and Outcome with Azathioprine Therapy Lewis et al. Gastroenterology 2000;118(6): 1018-24
The Value of a Short Term Trial • Define whether patient will respond to therapy • Entails limited risk • Pr(lymphoma)=(1/2000p-y) x (.25 p-y) = 1.25 per 10,000 subjects treated for 3 mos • Only continue therapy if there is documented benefit • Risk of long term therapy weighed against greater probability of benefit
Hepatosplenic T Cell Lymphoma • Reports to FDA AERS among patients with IBD1 • Thiopurine alone 17 • Anti-TNF alone 1 • Combination therapy 23 • Characteristics2 • Median age 22.5 (12 – 58) • 93% male • Median time since initiation of thiopurines ~6 years • Deepak P. Am J Gastroenterol 2013; 108:99–105 • Kotlyar D. Clin Gastroenterol Hepatol 2011;9:36–41
HSTCL Incidence • Kaiser Permanente Northern California • 6 cases from 2000 - 2006 • Overall 0.03 / 105 person-years • Men 0.04 / 105 person-years • Women 0.01 / 105 person-years • IBD – 1 case from 3,652 py of thiopurine exposure (patient also had anti-TNF exposure) • CESAME – 0 cases from 26,640 person-years (16,659 currently exposed, 9,981 prior exposure; 44% male) Herrinton LJ. Pharmacoepidemiol Drug Saf 2012; 21: 49–52 Beaugerie L. Lancet 2009;374:1617-1625
CESAME + KPNC • 1 case • 20,311 person-years of current exposure • 44% male in CESAME, KPNC unknown • Overall – 4.9 per 100,000 person-years • Male – 11.2 per 100,000 person-years Herrinton LJ. Pharmacoepidemiol Drug Saf 2012; 21: 49–52 Beaugerie L. Lancet 2009;374:1617-1625
Number Needed to Harm ‡ Kandiel A et al. Gut. 2005:54:1121-25 * 5 year survival = 68% for NHL, 85% for HD, estimated at 75% for this example † Estimated from KPNC (Herrinton LJ. Pharmacoepidemiol Drug Saf 2012; 21: 49–52) and CESAME (Beaugerie L. Lancet 2009;374:1617-1625)
NNH With and Without HSTCL This is almost certainly an over estimate of HSTCL incidence as it suggests that approximately 30% of lymphomas that occur among young males treated with thiopurines are HSTCL ‡ Kandiel A et al. Gut. 2005:54:1121-25 * 5 year survival = 68% for NHL, 85% for HD, estimated at 75% for this example † Estimated from KPNC (Herrinton LJ. Pharmacoepidemiol Drug Saf 2012; 21: 49–52) and CESAME (Beaugerie L. Lancet 2009;374:1617-1625)
Hazards of Modes of Transportation Cohen JT. Health Affairs 2007:26:636-46
Clinical Questions • Does immunosuppressant therapy increase the risk of lymphoma? • Thiopurines – yes, but risk may revert after discontinuation • TNF – Possibly • Combination – Yes and “probably” more than monotherapy • Do the benefits outweigh the risks? • In most scenarios • Is there anything I can do to decrease the risk of lymphoma?
Theory Behind Monitoring EBV Titers EBV Associated Lymphoma Acute Infection Early Rise EBV viral load Immunosuppression Recovery Recovery Time Adapted from Gulley LM. Clin. Microbiol. Rev. 2010, 23(2):350-66
Why does immunosuppression matter? • Immune surveillance • Epstein-Barr virus associated lymphoma * P<0.05 vs control. # P<0.05 vs. AZA and 5-ASA Percent of patients # # * Dayharsh GA. Gastroenterology 2002:122:72-77. Magro F. Inflamm Bowel Dis. 2013;19:1710-6
Decreasing the risk • Minimize unnecessary immunosuppression • What defines unnecessary immunosuppression? • Is there a role for discontinuing therapy in the setting of long term remission? • What is the minimum dose of thiopurines or methotrexate needed to augment effectiveness of anti-TNF drugs? • Is methotrexate less “lymphomagenic” than thiopurines and equally effective • EBV serology testing prior to treating • Monitoring EBV titers
Teens - 20s: High Risk Period for Infection Niederman JC. N Eng J Med 1970;282:361-5
Greater Risk of PTLD in Children, Elderly, and EBV Seronegative Risk factors for PTLD in adult kidney transplant recipients Gulley LM. Clin. Microbiol. Rev. 2010, 23(2):350-66 Caillard SC. Am. J. Transplant 2006;6:2735-42
EBV Serology • What we know • EBV infection is very common and typically occurs early in life1 • Seronegative transplant recipients have a higher risk of PTLD2 • De novo infection while immunosuppressed associated with higher incidence of lymphoma3 • Should we test EBV serologies prior to treatment in young patients and withhold thiopurines if EBV seronegative? 1. NiedermanJC. N Eng J Med 1970;282:361-5 2. CaillardSC. Am. J. Transplant 2006;6:2735-42 3. Ho M. J Infect Dis. 1985; 152(5): 876–886
Pros and Cons • No proven early interventions to prevent PTLD (e.g. antiviral agents) • Early detection of PTLD associated with better outcomes • More favorable histology / genetic profile Gulley LM. Clin. Microbiol. Rev. 2010, 23(2):350-66 Styczynski J. Bone Marrow Transplant 2009 May;43:757-70.
Guidelines on monitoring • Some organ and BM transplant guidelines recommend early aggressive monitoring in high risk patients • EBV mismatch, splenectomy, T cell depletion, use of ATG or OKT3 • No guidelines for IBD • Unlikely to be cost-effective (or feasible?) for IBD given lower risk of EBV-related lymphoma Gulley LM. Clin. Microbiol. Rev. 2010, 23(2):350-66 Styczynski J. Bone Marrow Transplant 2009 May;43:757-70.
Take Home Points • Thiopurines and possibly anti-TNF therapies increase the risk of lymphoma • A short trial of therapy has little long term risk of lymphoma and can inform the risk-benefit balance of long term therapy • Discontinue ineffective medications unless can justify for other reason, e.g. preventing antibody formation • Additional caution may be warranted in young EBV serology negative patients, young males and the elderly