Download
1 / 1
10 likes | 82 Views
Figure 1. Diagnostic plots for propofol pharmacokinetics and effect (BIS) in morbidly obese patients including observations versus individual-predictions (A) and observations versus population-predictions (B). PK-Final Total Body Weight model PD-Final model.

E N D
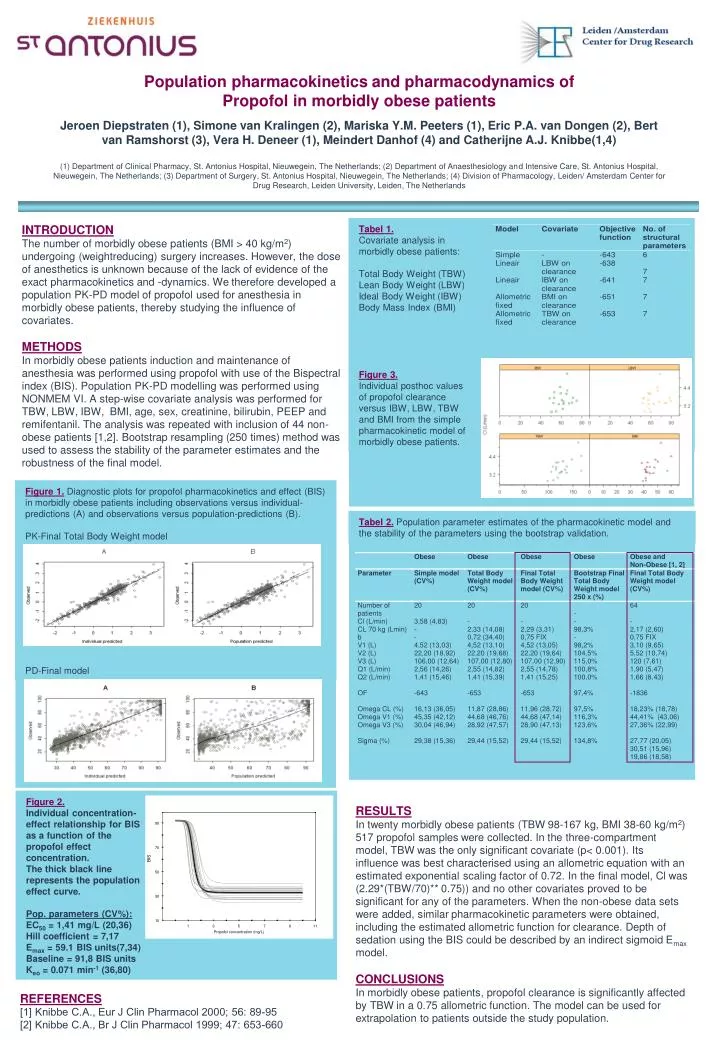
Figure 1.Diagnostic plots for propofol pharmacokinetics and effect (BIS) in morbidly obese patients including observations versus individual-predictions (A) and observations versus population-predictions (B). PK-Final Total Body Weight model PD-Final model Tabel 2.Population parameter estimates of the pharmacokinetic model and the stability of the parameters using the bootstrap validation. Figure 2. Individual concentration- effect relationship for BIS as a function of the propofol effect concentration. The thick black line represents the population effect curve. Pop. parameters (CV%): EC50 = 1,41 mg/L (20,36) Hill coefficient = 7,17 Emax = 59.1 BIS units(7,34) Baseline = 91,8 BIS units Keo = 0.071 min-1 (36,80) Tabel 1. Covariate analysis in morbidly obese patients: Total Body Weight (TBW) Lean Body Weight (LBW) Ideal Body Weight (IBW) Body Mass Index (BMI) Figure 3. Individual posthoc values of propofol clearance versus IBW, LBW, TBW and BMI from the simple pharmacokinetic model of morbidly obese patients. Population pharmacokinetics and pharmacodynamics of Propofol in morbidly obese patientsJeroen Diepstraten (1), Simone van Kralingen (2), Mariska Y.M. Peeters (1), Eric P.A. van Dongen (2), Bert van Ramshorst (3), Vera H. Deneer (1), Meindert Danhof (4) and Catherijne A.J. Knibbe(1,4)(1) Department of Clinical Pharmacy, St. Antonius Hospital, Nieuwegein, The Netherlands; (2) Department of Anaesthesiology and Intensive Care, St. Antonius Hospital, Nieuwegein, The Netherlands; (3) Department of Surgery, St. Antonius Hospital, Nieuwegein, The Netherlands; (4) Division of Pharmacology, Leiden/ Amsterdam Center for Drug Research, Leiden University, Leiden, The Netherlands INTRODUCTION The number of morbidly obese patients (BMI > 40 kg/m2) undergoing (weightreducing) surgery increases. However, the dose of anesthetics is unknown because of the lack of evidence of the exact pharmacokinetics and -dynamics. We therefore developed a population PK-PD model of propofol used for anesthesia in morbidly obese patients, thereby studying the influence of covariates. METHODS In morbidly obese patients induction and maintenance of anesthesia was performed using propofol with use of the Bispectral index (BIS). Population PK-PD modelling was performed using NONMEM VI. A step-wise covariate analysis was performed for TBW, LBW, IBW, BMI, age, sex, creatinine, bilirubin, PEEP and remifentanil. The analysis was repeated with inclusion of 44 non-obese patients [1,2]. Bootstrap resampling (250 times) method was used to assess the stability of the parameter estimates and the robustness of the final model. RESULTS In twenty morbidly obese patients (TBW 98-167 kg, BMI 38-60 kg/m2) 517 propofol samples were collected. In the three-compartment model, TBW was the only significant covariate (p< 0.001). Its influence was best characterised using an allometric equation with an estimated exponential scaling factor of 0.72. In the final model, Cl was (2.29*(TBW/70)** 0.75)) and no other covariates proved to be significant for any of the parameters. When the non-obese data sets were added, similar pharmacokinetic parameters were obtained, including the estimated allometric function for clearance. Depth of sedation using the BIS could be described by an indirect sigmoid Emax model. CONCLUSIONS In morbidly obese patients, propofol clearance is significantly affected by TBW in a 0.75 allometric function. The model can be used for extrapolation to patients outside the study population. REFERENCES [1] Knibbe C.A., Eur J Clin Pharmacol 2000; 56: 89-95 [2] Knibbe C.A., Br J Clin Pharmacol 1999; 47: 653-660






















