Download
1 / 50
500 likes | 652 Views
Cardiac Conditions. Fred Reifsteck MD Head Team Physician University of Georgia. What is the leading cause of death in the United States for men and women?. Congenital Cardiac Conditions. Hypertrophic Cardiomyopathy Coronary Artery Anomalies Marfan’s Syndrome Long QT Syndrome.

E N D
Cardiac Conditions Fred Reifsteck MD Head Team Physician University of Georgia
What is the leading cause of death in the United States for men and women?
Congenital Cardiac Conditions Hypertrophic Cardiomyopathy Coronary Artery Anomalies Marfan’s Syndrome Long QT Syndrome
Acquired Cardiac Conditions Hypertension Coronary Artery Disease
Congenital Problems Concerns about sudden cardiac death Problem may not be discovered until death or autopsy Symptoms include chest pain, exertional dyspnea, or syncope
Sudden Cardiac death in Athletes (2005) High school and college women 1/769,000 High school and college men 1/133,00 Males > 40 yrs. Old risk of SCD increases 8-56 times with exercise Approximately 0.2% of athletes have CV conditions that could predispose them to SCD Syncope precedes sudden cardiac death in 17 to 50 % of athletes and precedes exercise related sudden cardiac death in 80% of athletes
Preparticipation Screening Incidence of sudden cardiovascular death in young competitive athletes has decreased in the Veneto region of Italy since the introduction of nationwide systemic screening. It lowered the incidence of death from cardiac pathology. USA has a DIFFERENT ethnic and genetic composition
Dynamic: Isotonic Static: Isometric Clearing athlete with a particular condition may depend on their sport. Golf Low dynamic, Low static Basketball High Dynamic, Moderate static
Disclaimer Knowledgeable and reasonable cardiologists may read the same literature and review the same guidelines with regard to the same patient data (history, physical exam, test results) and arrive at very different conclusions with regard to determining eligibility for competitive sports.
Hypertrophic Cardiomyopathy • Heterogeneous left ventricle hypertrophy and wall thickening associated with a non-dilated cavity in the absence of another cardiac or systemic disease. Left atrial enlargement. • Primary and familial cardiac malformation with disease causing mutations in 10 genes encoding sarcomeric and regulatory proteins. • Two types • Obstructive • Nonobstructive
Physical Exam In nonobstructive type, murmur may be absent or decreased. Obstructive type classic murmur, harsh mid systolic left lower sternal border, increases with standing or valsalva
Detectection on Preparticipation Screening • History: Exertional syncope; family history of HCM or premature cardiac death • Noninvasive testing: ECG, ECHO which shows wall thickness greater than 15 mm. May be falsely negative if there is incomplete physiologic expression • Gene testing
Eligibility to Participate, 36 th Bethesda Conference Athletes with a probable or unequivocal clinical diagnosis of HCM should be excluded from most competitive sports, with the possible exception of those of low intensity. This recommendation is independent of age, gender, and physiologic appearance, and does not differ for those athletes with or without symptoms, LV outflow obstruction, or prior treatment with drugs, or major interventions with surgery, alcohol septal ablation, pacemaker, or implantable defibrillator. Although the clinical significance and natural history of genotype positive- phenotype negative individuals remains unresolved, no compelling data are available at present with which to preclude these patients from competitive sports, particularly in the absence of cardiac symptoms or a family history of sudden death.
Coronary Artery Anomalies Pete Maravich died from this condition Second leading cause of SCD Most common variant left main and right coronary arise from right sinus of valsalva Single right coronary and absent left artery was what Pete Maravich had Exercise leads to decreased cardiac muscle perfusion, ischemia, ventricular arrhythmias May have chest pain, dyspnea, syncope with exertion About ½ of people have syncope in the weeks prior to death
Detection on Preparticipation Screening If symptomatic diagnosis by ECHO and catherization Coronary CT can quickly and unambiguously define the coronary anatomy in a 3 D representation. Should be considered the gold standard when an anomaly is suspected in an athlete
Eligibility to Participate Detection should result in exclusion from all participation in competitive sport Participation in sports greater than six months after operative repair is permitted if the athlete does not have ischemia on maximal exercise testing
Marfan’s Syndrome Autosomal dominant disorder of the connective tissue Aortic root dilation and eventual rupture the cause of death
Physical Exam Tall stature Long digits, limbs Laxity of joints Pectus excavatum Ectopic lens With significant aortic root dilation and regurgitation there is a midsysolic click, followed by a late systolic murmur
Special attention to other physical exam findingsECHO for aortic root dilation
Eligibility to Participate Athlete can participate in low and moderate static/ low dynamic competitive sports with NO aortic root dilation; moderate-to-severe mitral regurgitation; family history of dissection or sudden death. Needs follow up ECHO every 6 months Unequivocal aortic root dilation, prior root surgical reconstruction, chronic dissection, moderate-to-severe mitral regurgitation, or a family history of dissection or sudden death can participate in low intensity competitive sports Not participate in sports with potential for bodily collision
Long QT Syndrome Inherited disorder that leads to prolongation of ventricular repolarization and is associated with malignant arrhythmia. First event may be syncope, nonfatal Female predominance Genotype is important (gene studies) 3 important factors for estimating the risk of life threatening events with suggested LQTS A) Timing and frequency of recurrent syncope B) Duration of the QTc interval C) Sex
Detection on Preparticipation Screening ECG:QT interval corrected for heart rate, 0.44 seconds in males; 0.46 seconds in females Roughly 3 + big boxes, 18-20 small boxes on the ECG
Eligibility to Participate Perhaps low static/ low dynamic especially with implanted defibrillator (ICD)
Acquired problems Conditions that are predominantly caused by lifestyle choices: diet, obesity, smoking, alcohol, drugs, physical inactivity Genetics can play a role Work on prevention before treatment Huge health care expenditure Epidemic of childhood obesity
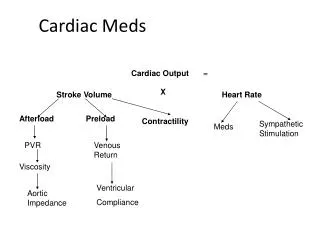
Hypertension BP = cardiac output (CO) x total peripheral resistance (TPR) JNC VII (Joint National Committee on the Prevention, Detection, Evaluation and Treatment of High Blood Pressure) Added prehypertension 121-139/ 81-89
The Fourth report Used for children Prehypertension: systolic or diastolic from the 90 th to just below the 95 th percentile Stage 1: between 95 th and 99 th percentile plus 5 mm Hg Stage 2: > 95 th percentile plus 5 mm Hg Athlete with sustained hypertension is now recommended by Fourth report as well as 36 th Bethesda Conference to have an ECHO and to limit participation until BP is normalized
Systolic Diastolic Normal <120 <80 Prehypertension 120-129 85-89 Stage 1 140-159 90-99 Stage 2 160 100 Most hypertension is essential, multifactorial Non essential, type 2, identifiable causes: sleep apnea, renal artery stenosis
Physical Exam Family history Check BP both arms, legs Heart exam Pulses Lungs Fundoscopic exam CBC, U/A, Thyroid ? CXR ?ECG
Detection on Preparticipation Screening Look at the vital signs Examine the patient, probably not mass screenings
Eligibility to participate Prehypertension, Stage 1: allow to play if BP is well controlled and there is no target organ damage or heart disease. Consider lifestyle modifications, and drug therapy Stage 2: restrict from play especially in sports with a high static component until hypertension is controlled
Coronary Artery Disease Most common cause of exercise related cardiac events and sudden death in adults especially older than 30 Commonly causes angina pectoris, myocardial infarction
Mechanism Fatty streaks Accumulation of extracellular lipids Recruitment of leukocytes, adhesive molecules Eventual formation of plaque which has a necrotic core Acute rupture can lead MI, death Prevention is risk factor modification
Physical Exam History especially comorbid conditions (diabetes) or family history Vital signs, esp. BP Cardiac exam Labs: lipids, blood sugar, kidney
Detection on Preparticipation Screening ECG ? Old changes Stress testing prior to starting vigorous exercise at age 40.
Eligibility to participate Athletes with documented advanced coronary disease should generally be restricted to low intensity competitive events Athletes with reduced exertional capacity but without advanced coronary artery disease can participate in sports in accordance to their capacity Athletes without advanced coronary disease and with normal exercise tolerance for age can generally participate in competitive sports
Commotio Cordis Concussive injury to the heart resulting in ventricular dysrhythmia and cardiac asystole Ventricular fibrillation is the most commonly associated arrhythmia Most common sports baseball, softball, hockey and lacrosse Survival is low even with resuscitative equipment No evidence of heart injury at autopsy
Arrhythmogenic Right Ventricular Dysplasia Morphologic fibrofatty replacement and thinning of right ventricular wall Most common cause of sudden cardiac death in Italy 3:1 male ratio Palpitations, fatigue, syncope ECG T wave inversion; VT with a LBBB Endomyocardial biopsy Progressive disease Athletes with probable or definite diagnosis of disease should be excluded from most competitive sports with possible exception of low intensity class
Heart disease is especially common Need to evaluate may exist from childhood to senior years ? Best cost effective screening Be watchful for conditions, some preventable and some are not