Download
1 / 15
160 likes | 389 Views
Minimally Invasive Follicular Carcinoma: A Cytological and Histological Challenge. David Poller, Queen Alexandra Hospital,Portsmouth , UK. 22 year old female euthyroid , T4 11.3 (N 7.0-20), TSH 0.81 (N 0.35-5.0), Ab – ve MNG, ultrasound guided FNA of a large 29mm solid nodule in left lobe.

E N D
Minimally Invasive Follicular Carcinoma: A Cytological and Histological Challenge David Poller, Queen Alexandra Hospital,Portsmouth, UK
22 year old female euthyroid, T4 11.3 (N 7.0-20), TSH 0.81 (N 0.35-5.0), Ab –ve • MNG, ultrasound guided FNA of a large 29mm solid nodule in left lobe
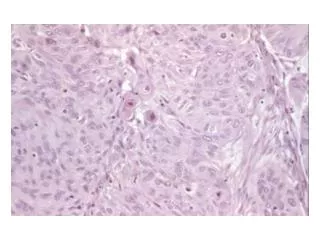
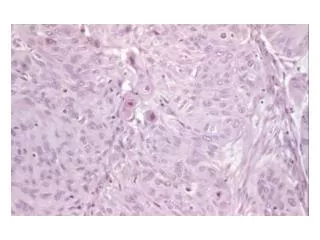
Cytology • US guided FNA, 4 slides, air dried pap & giemsawithout rapid on site assessment • Moderate cellularity, virtually no colloid, some cell clusters 3 dimensional with some nuclear features suggestive of papillary carcinoma; Thy4 ~Bethesda V, • Multidisciplinary team decision->left thyroid lobectomy
Diagnosis Thy4 = Bethesda Class V suspicious neoplasm, cannot exclude FVPC Left thyroid lobectomy = 20g Minimally invasive well differentiated follicular carcinoma, a 42mm pT3 well differentiated follicular carcinoma, foci of vascular invasion-> completion thyroidectomy
Minimally Invasive Follicular Carcinoma • Requires assessment of whole lesion with capsule & surrounding thyroid • WHO 2004 definition = transcapsular invasion or vascular invasion
. What is Invasion?? ‘..Our review of the anatomy of the thyroid gland con-firms that this structure has no defined anatomical fibrous capsule..’ ‘..We suggest that the criteria for diagnosing angioinvasion in thyroid carcinomas as well as in other endocrine tumors are inconsistent. ..’ 4000 carcinoma cases, very rigid criteria 118 cases with tumour invading vessel wall & thrombus adherent to intravascular tumour, 35% developed distant metastases at mean 5.3y follow up
Minimal Invasion ‘..The importance of the study is the confirmation that diagnostic reproducibility of minimally invasive FTC is low and that this has clinical implications, and also implications for the design of studies into the treatment and outcome of FTC’
Garcia-Rostan & Sobrinho-Simões Diagn Histopathol 2011; 17: 119.
Other Systems • Veracyte: Alexander et al NEJM 2012 mRNA needle washings, 265 nodules, high negative predictive value, 8% misclassified as benign, BUT low +ve predictive value for malignancy, 48% of benign nodules classified as suspicious, cost US$ 3200 per test • AssuragenmiRInform: Braf, Ret/Ptc, Ras, Pax8/PPARg, specificity 98%, sensitivity 60% Hodak & Rosenthal Thyroid 2013, cost US $650 per test
Finally • The criteria for maligancy in follicular lesions are not precise and some follicular thyroid lesions with genotypes of follicular carcinomas may well be ‘in situ’ lesions that do not demonstrate invasion using conventional morphological criteria • If you want to diagnose thyroid nodules you need representative cells from the lesion(s) • But in many cases Class I and Class III aspirate rates are high; eg Class 1 up to 15%+ and Class III up to 20%, often because of poorly prepared slides lacking cells • Rapid On Site Assessment is Essential