Download

1 / 13
130 likes | 317 Views
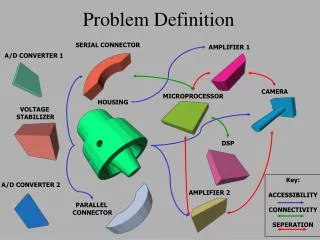
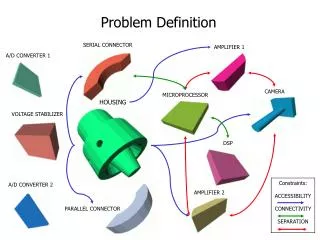
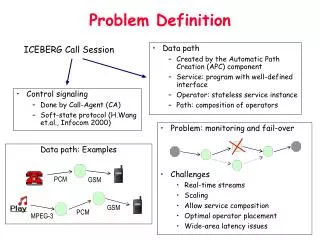
Problem Definition. 19y/o previously healthy male with concerning social hx Subacute onset progressive fatigue, weakness, paresthesias , dysphagia , hoarse voice Exam findings of symmetric weakness and decreased DTR’s, facial weakness, NIF’s c/w respiratory compromise

E N D
Problem Definition • 19y/o previously healthy male with concerning social hx • Subacute onset progressive fatigue, weakness, paresthesias, dysphagia, hoarse voice • Exam findings of symmetric weakness and decreased DTR’s, facial weakness, NIF’s c/w respiratory compromise • Also with vomiting, ulcerative gingivitis, wt loss
Illness Script • Acute to subacute, rapidly progressive, symmetric ascending muscle weakness, lack of deep tendon reflexes, with prodromal viral illness.
Guillian-Barre • Heterogeneous syndrome with several variant forms • Demyelinating (classic) vs. axonal • AIDP: Acute inflammatory demyelinatingpolyradiculopathy
Guillian-Barre: Pathophysiology • Immune-mediated condition of peripheral nervous system • Pathogen shares similar antigenic sites as host axon or peripheral nerve myelin • Autoimmune response • Multifocal areas of inflammation, especially at spinal roots and peripheral nerves • Demyelination from macrophages invading basement membrane of Schwann cells
Pathophysiology • Demyelination results in conduction block and flaccid paralysis • Inflammation leads to breakdown of blood-brain barrier • Transudation of plasma proteins into CSF
Prodromal Pathogens • CMV, EBV, other herpesviruses, HIV • Campylobacter jejuni, typhoid, paratyphoid, listeria, Mycoplasma pneumonia • Vaccines • Surgery
Clinical Features • All ages, rare in infants • Three phases: • Progressive • Plateau • Resolution • Miller-Fisher syndrome • Ophthalmoplegia, areflexia, ataxia
Clinical Features • Cranial nerves in 33% (Facial most common) • Sensory disturbance frequent • Pain or paresthesiasof extremeties, back, perioral • Only minimal loss of sensation • Autonomic dysfunction • Tachycardia, bradycardia, HTN, orthostatic hypotension • Rare bowel and bladder dysfunction
Studies • CSF “Cytoalbuminemic disassociation” • Elevated protein • <10 WBC with monocyte predominance • Electrodiagnostic studies aid in dx
Management • ABC’s • Supportive care • Intubation (20%) • CPT • IVIG daily X 5 days • Plasmapheresis equal efficacy • Physical therapy • Steroids not shown to help
Morbidity/Mortality • Causes of death • Autonomic dysfunction • Respiratory failure • 23% residual weakness at least 1 muscle group • Minimal impact on function • Long term weakness associated with • Younger age at onset (<9) • Rapid progression to maximal weakness • May progress to Chronic Inflammatory Demyelinating Neuropathy