Download
1 / 21
210 likes | 306 Views
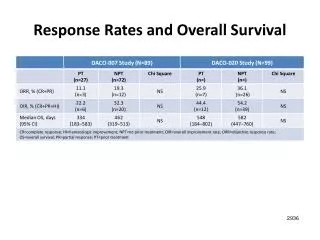
OVERALL SURVIVAL. 100 95 90 85 0. Simvastatin (n=2221). Placebo (n=2223). % of patients alive. 30% risk reduction P=0.0003. 0 1 2 3 4 5 6. Years since randomization. Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389. CORONARY MORTALITY. 200

E N D
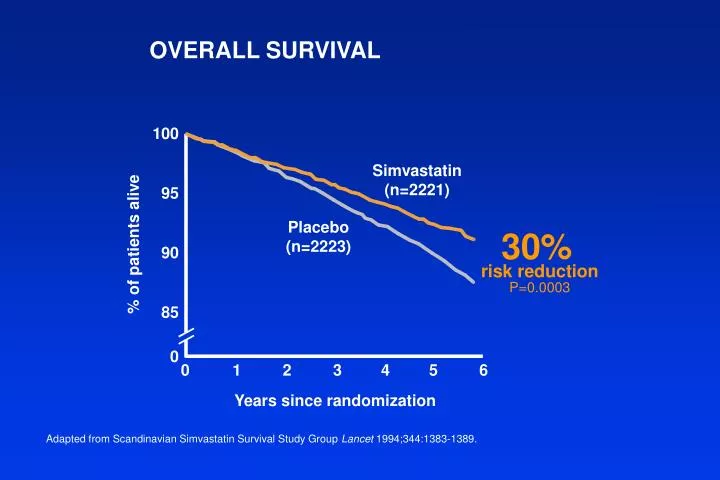
OVERALL SURVIVAL 100 95 90 85 0 Simvastatin(n=2221) Placebo(n=2223) % of patients alive 30% risk reduction P=0.0003 0 1 2 3 4 5 6 Years since randomization Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
CORONARY MORTALITY 200 150 100 50 0 189 No. of deaths 111 42% risk reduction P=0.00001 Placebo(n=2223) Simvastatin(n=2221) Adapted from Kjekshus J et al Am J Cardiol 1995;76(9):64C-68C.
CAUSES OF MORTALITY 11.5% 8.2% Coronary Othercardiovascular Cancer Other Placebo(n=2223) Simvastatin(n=2221) Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
MAJOR CORONARY EVENTS Coronary Death or Nonfatal MI 100 90 80 70 0 Simvastatin(n=2221) % of patients without events Placebo(n=2223) 34% risk reduction P <0.00001 0 1 2 3 4 5 6 Years since randomization Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
CORONARY EVENTS VS. BASELINE LDL Coronary Deaths or Nonfatal MIs by Baseline LDL-C Quartiles 40 35 30 25 20 15 10 5 0 36% 35% 33% 32% % risk reduction <4.39 mmol/L (170 mg/dl) 4.40–4.84 mmol/L (170–187 mg/dl) 4.85–5.34 mmol/L (188–207 mg/dl) >5.35 mmol/L (207 mg/dl) Baseline LDL-C Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1995;345(8960):1274-1275.
SUBGROUP COMPARISON –MAJOR CORONARY EVENTS Coronary Death and Nonfatal MI 33.4 35 30 25 20 15 10 5 0 29.5 Placebo Simvastatin 26.4 23.6 21.7 20.5 18.1 14.7 % of patients Men 34% risk reduction Women 34% risk reduction Age <65 34% risk reduction Age >65 34% risk reduction Adapted from Miettinen TA et al Circulation 1997;96:4211-4218.
CORONARY EVENT REDUCTION Simvastatinbetter Placebobetter Age Gender Smoking Hypertension Diabetes <60 yrs 60–70 yrs Men Women Yes No Yes No Yes No P <0.0001 P <0.0001 P <0.00001 P=0.01 P=0.00105 P=0.00009 P=0.00006 P <0.00001 P <0.00169 P <0.000001 0.2 0.4 0.6 0.8 1.0 1.2 Relative risk (95% Cl) Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389; Kjekshus J et al Am J Cardiol 1995;76(9):64C-68C; Data on file, MSD.
MI REDUCTION Myocardial Infarction 600 500 400 300 200 100 0 562 369 No. of patients 37% risk reduction P <0.00001 Placebo(n=2223) Simvastatin(n=2221) Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389; Data on file, MSD.
NEED FOR PTCA/CABG 100 90 80 0 Simvastatin(n=2221) % of patients withoutPTCA or CABG 37% risk reduction P <0.00001 Placebo(n=2223) 0 1 2 3 4 5 6 Years since randomization PTCA = percutaneous transluminal coronary angioplasty; CABG = coronary artery bypass graft Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
HOSPITAL DAYS Cardiovascular Hospital Days 16,000 12,000 8000 4000 0 15,089 9951 No. of cardiovascularhospital days 34% reduction P <0.0001 Placebo(n=2223) Simvastatin(n=2221) Adapted from Pedersen TR et al Circulation 1996;93(10):1796-1802.
ATHEROSCLEROSIS • Coronary arteries • Carotid arteries • Femoral arteries Atherosclerosis is a widespread disease affecting all vascular beds including
STROKE/TIA 6 5 4 3 2 1 0 Placebo(n=2223) 28% risk reduction P=0.033 % of patients Simvastatin(n=2221) 0 1 2 3 4 5 6 Years Adapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
CAROTID BRUITS* 2.5 2.0 1.5 1.0 0.5 0 Placebo(n=2223) 48% risk reduction P=0.009 % of patients Simvastatin(n=2221) 0 1 2 3 4 5 6 Years *A post-hoc analysis of 4S Adapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
INTERMITTENT CLAUDICATION* New or Worsening Intermittent Claudication 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0 Placebo(n=2223) 38% risk reduction P=0.008 % of patients Simvastatin(n=2221) 0 1 2 3 4 5 6 Years *A post-hoc analysis of 4S Adapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
ANGINA PECTORIS* New or Worsening Angina Pectoris 40 35 30 25 20 15 10 5 0 Placebo(n=2223) 26% risk reduction P<0.0001 % of patients Simvastatin(n=2221) 0 1 2 3 4 5 6 Years *A post-hoc analysis of 4S Adapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
DEVELOPMENT OF HEART FAILURE 100 98 96 94 92 90 0 Simvastatin(n=2221) % without CHF Placebo(n=2223) 21% risk reduction P <0.015 6 12 18 24 30 36 42 48 54 60 66 72 Months since randomization Adapted from Kjekshus J et al J Card Fail 1997;3(4):249-254.
CHOLESTEROL PARAMETERS Simvastatin 20 mg, Week 6 20 10 0 –10 –20 –30 –40 +8% P <0.0001 –15% Mean % change –28% –38% LDL-C Total C HDL-C Triglycerides Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389; Data on file, MSD.
PATIENT FOLLOW-UP Placebo Simvastatin (n=2223) (n=2221) Lost to follow-up 0% 0% Treatment discontinuations 13% 10% Adverse effects 6% 6% Personal reasons/other 7% 5% Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
TRANSAMINASES AND CK Elevations Occurring More than Once during 5.4 Years of Therapy Placebo Simvastatin No. (%) No. (%) AST >3 ULN 7 (0.3) 5 (0.2) ALT >3 ULN 12 (0.6) 14 (0.7) CK >10 ULN 0 0 AST = aspartate aminotransferase; ALT = alanine aminotransferase; CK = creatine kinase; ULN = upper limit of normal Adapted from Pedersen TR et al Arch Intern Med 1996;156:2085-2092.
CONCOMITANT CARDIOVASCULARTHERAPY – BASELINE Simvastatin Placebo 20–40 mg Drug Class/Therapy No. No. Aspirin 815 822 Beta blockers 1266 1258 Calcium antagonists 668 712 Isosorbide mono/dinitrate 727 684 Thiazides 138 151 Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
LONG-TERM SAFETY • Simvastatin had an excellent five-year safety profile • Adverse experiences similar to placebo • Only one reversible case of myopathy reported • Incidence of liver enzyme elevations similar to that of placebo • No interactions reported with beta blockers, calcium-channel blockers, aspirin, and thiazides • No increase in cancer overall or at any particular site • No previously unrecognized adverse effects observed 4S provided the largest and longest follow-up of patients treated with simvastatin (5.4 median years) Adapted from Pedersen TR et al Arch Intern Med 1996;156:2085-2092.