Download

1 / 60
600 likes | 624 Views
COMMON ENDEMIC INFECTIOUS DISEASES IN SAUDI ARABIA. MAP. BRUCELLOSIS. MICROBIOLOGY. 6 SPECIES, 4 CAN BE TRANSMITTED TO MAN. GRAM NEGATIVE, NON-MOTILE, NON-SPORE FORMING. THE ORGANISM IS FACULATIVE. CULTURE CAN TAKE LONG TIME. SURVIVAL CAN BE VERY LONG.

E N D
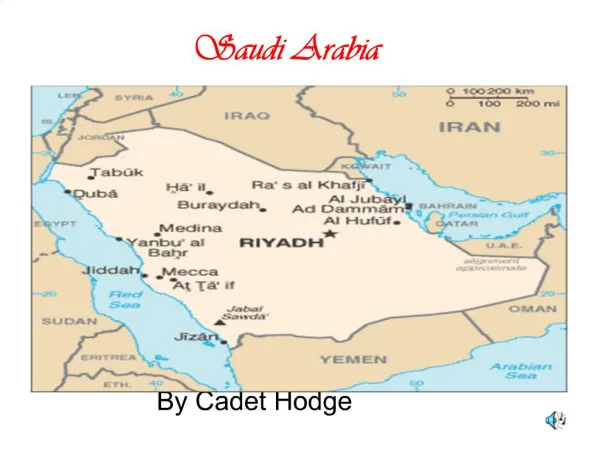
COMMON ENDEMIC INFECTIOUS DISEASES IN SAUDI ARABIA
MICROBIOLOGY • 6 SPECIES, 4 CAN BE TRANSMITTED TO MAN. • GRAM NEGATIVE, NON-MOTILE, NON-SPORE FORMING. • THE ORGANISM IS FACULATIVE. • CULTURE CAN TAKE LONG TIME. • SURVIVAL CAN BE VERY LONG. • OPTIMUM TEMPERATRE IS 37 °C (20-40 °C)
REGIONAL DISTRIBUTION OF SEROPOSITIVITY ACCORDING TO THE MICROPLATE AGGLUTINATION TEST
Prevalence of Brucellosis in Al-Qaseem Area Al-Balla S.R. Unpublished data
PMN T Suppresser Ant. Pr. Cell T. helper B cell Macrophage Elimination OR
AFTER ENTERING THE BODY Leukocyte OR Regional Lymph node OR Blood Stream Liver Spleen Bone Marrow Lymph Node OR Microgranuloma Micro abscess formation OR OR Blood Stream BLOOD STREAM BLOOD STREAM BLOOD STREAM
SEROLOGICALTESTS • STANDARD TUBE AGGLUTINATION TEST • MICROPLATE AGGLUTINATION TEST • 2-MERCAPTOETHANOL AGGLUTINATION TEST • COOMBS TEST • COMPLEMENT FIXATION TEST • ROSE BENGAL TEST • ENZYME-LINKED IMMUNOSORBENT ASSAY • GEL PRECIPITAITON TEST
ACTIVE DISEASE • Clinical evidence (symptoms & signs) of brucellosis plus: • Positivity at > 1:160 by STAT • Positivity at > 1:140 by 2-ME test • Positivity by ELISA (high IgG & low IgM)
VACCINES • B. abortus strain 19 • B. melitensis strain Rev I • B. suis strain 2s • B. abortus strain 45/20 • B. melitensis strain H38
PREVENTION • “ELIMINATION OF THE DISEASE IN ANIMALS” • PERSONAL HYGIENE (WASHING EXPOSED CLOTHES) • ENVIRONMENTAL SANITATION (DISPOSAL OF CONTAMINATED SUBSTANCES) • PASTURIZATION OF DIARY PRODUCTS • HEALTH EDUCATION • IMMUNIZATION
PREVALENCE OF SCHISTOSOMIASIS AS REPORTED BY THE STATION __________________________________________ Prevalence (%) No. of Overall Persons S. Haema- S.Man- Preva Station Examined tobium soni lence+ ____________________________________________ Al Baha 20.142 -- 13.0 13.0 Jizan 30.883 7.0 1.2 8.2 Taif 39.559 0.2 7.7 7.9 Abha 23.013 1.7 4.9 6.6 Madinah 17.591 1.9 3.6 5.5
Prevalence (%) No. of Overall Persons S. Haema- S.Man- Preva Station Examined tobium soni lence+ ____________________________________________ Bisha 16.766 0.4 8.5 8.9 Najran 8.820 1.6 9.9 11.5 Mahael 5.783 7.6 --- 7.6 Hayil 4.335 --- 14.2 12.2 Riyadh 15.129 --- 5.6 5.6 Makkah 25.894 2.5 3.0 5.5 Al-Jouf 12.577 1.3 1.6 2.9
S P Inf. Mesentery Rectal
KATAYAMA FEVER(KATAYAMA River, Japan) • SEVERAL DAYS – 2-3 WEEKS • FEVER, CHILLS, HEADACHE, MALAISE, EDEMA, CONFUSION • HEPATOSPLENOMEGALLY • LYMPHADENOPATHY • EOSINOPHILIA • CEREBRAL EDEMA (CT)
What is the most serious common complication of Schistosomiasis infection?
Communication with Systemic Circulation
U SCHISTOSOMIASIS Kidney U. Bladder
SALMONELLA TYPHOID FEVER
CLASSIFICATION OF SALMONELLA • According to their ecologic niches • Serotyping [kanfmann white] • O antigen A-I • H antigen (subtypes) * Over 2000 serotypes
Spectrum of clinical manifestations of salmonella • Gastroenteritis • Enteric fever • Bacteremia • With metastatic disease • Without metastatic disease • Asymptomatic carrier state
S. PATHOGENESIS • ID 10ˆ6 – 10ˆ9 • Penetration of the distal ileum mucosa • Multiplication in the payer patches • Diarrhea is caused by: • Prostlaglandin Induced ˆ (c-AMP) • Local Inflamatory rasponce • S. enterotoxin
TYPHOID FEVER(Enteric Fever) • Definition: A disease characterized by prolonged fever, abdominal pain, diarrhea, delirium, rash (rose spots) & splenomegally. • Etiology: Salmonella Typhi & paratyphi A & B-A motile gram-negative bacilli, which possess: • H-Antigen (associated with flagella) • O-Antigen (a LPS associated with cell wall) • VI-Antigen (a PS associated with cell capsule)
EPIDEMIOLOGY OF TYPHOID FEVER • It affects all age groups. • No sex difference. • Common in developing countries. • Infecting dose 7x10(6) in Africa, Asia & Latin America. • Transmission is through Oral-fecal route. • Affected individuals may become asymptomatic carriers particularly females & older males (Underlying cholecystitis). • S-Typhi is resistant to drying & cooling.
SIGNS & SYMPTOMS(cont,) ______________________________________ Symptoms Signs Pathology _____________________________________________________________ 3rd wk Intestinal Melena Ulcerations, perforation bleeding, per- rigid abdomen with peritonitis. foration & shock ileus, coma ____________________________________________________________ 4th week Resolution Recurrence Cholecystitis, chronic & later relapse of acute fecal carriage of bacteria weight loss disease, cachexia.
ANTIBIOTIC USED FOR SALMONELLA TYPHI • Chloramphenicol • Ampicillin, Amoxil • Co-trimoxazole • 3rd generation cephalosporins • Quinolones
PROGNOSIS • Case fatality dropped 12% to 4% • It is still +\- 10% in developing countries • Perforation +\- 5% • Chronic fecal carriers 1-3%
VACCINATION FOR S.TYPHI • Inativated S.typhi: • 2 SC injections: • 55-88% protection for 3-5yr. • Attenuated S.typhi: • Liquid 3 doses • Enteric coated capsules • Protection 60-70%
LEISHMANIASIS It is the result of the infection with one of or other species of protozoa (leishmania). Conveyed by: Sandflies (Phlebotomus). Visceral Leishmaniasis: L. donovani Mucocutaneous : L. Braziliensis
Cutaneous : L.tropica major L. tropica minor New World : L. Braziliensis L. Mexicana Old world
PATHOLOGY » L. donovani parasitizes the reticu. endoth. cells » Great proliferation of macrophage » Cells result: Liver – spleen enlarg. » The red bone marrow extend. »
CLINICAL PICTURE • Incubation: 2 weeks – 18 months early stages is not easy for diagnose. There is no constant physical signs. BP , Pulse , - Fever ☺ Changes in the blood picture particularly Leucopenia. ☺ Outstanding physical sign is the enlargement of the spleen 3 cm. a month.
● Liver : enlarged spleen + liver are neither tender nor painful. ● Sometimes: Jaundice = prognost. Significance ● Enlarged : Lymph node, could be but its not a feature of the disease. ● Wasting : Emaciated pat with a protuberant