Download
1 / 1
10 likes | 70 Views
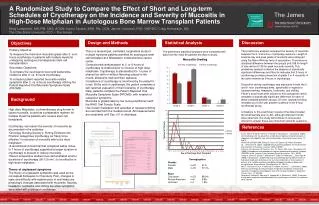
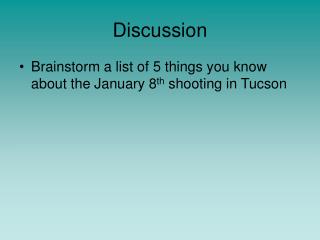
Importance of Color Doppler Imaging in the Diagnosis of Anomalous Coronary Artery Origin From Pulmonary Artery. Tharakanatha R. Yarrabolu, MD; Nazire Ozcelik, MD; Duraisamy Balaguru, MD University of Texas Health Science Center, Houston Texas. Introduction.

E N D
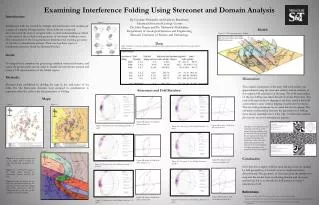
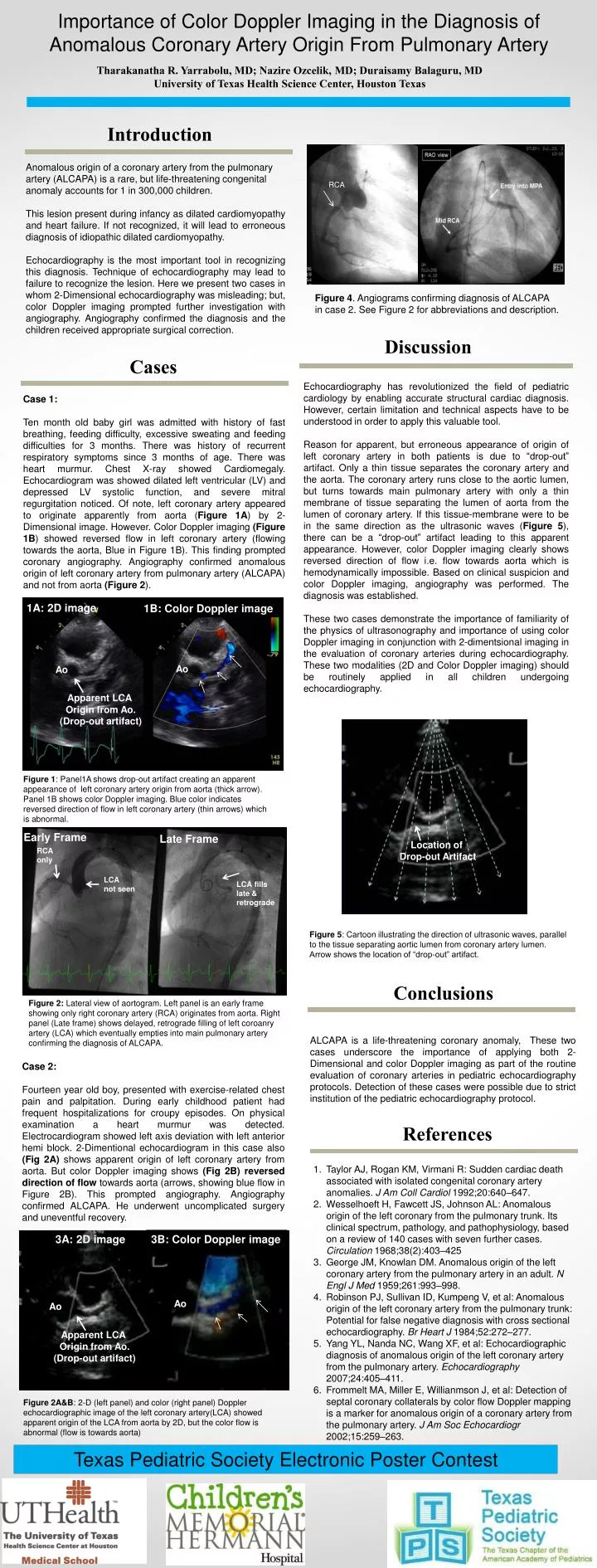
Importance of Color Doppler Imaging in the Diagnosis of Anomalous Coronary Artery Origin From Pulmonary Artery Tharakanatha R. Yarrabolu, MD; Nazire Ozcelik, MD; Duraisamy Balaguru, MD University of Texas Health Science Center, Houston Texas Introduction Anomalous origin of a coronary artery from the pulmonary artery (ALCAPA) is a rare, but life-threatening congenital anomaly accounts for 1 in 300,000 children. This lesion present during infancy as dilated cardiomyopathy and heart failure. If not recognized, it will lead to erroneous diagnosis of idiopathic dilated cardiomyopathy. Echocardiography is the most important tool in recognizing this diagnosis. Technique of echocardiography may lead to failure to recognize the lesion. Here we present two cases in whom 2-Dimensional echocardiography was misleading; but, color Doppler imaging prompted further investigation with angiography. Angiography confirmed the diagnosis and the children received appropriate surgical correction. RCA Figure 4. Angiograms confirming diagnosis of ALCAPA in case 2. See Figure 2 for abbreviations and description. Discussion Cases Echocardiography has revolutionized the field of pediatric cardiology by enabling accurate structural cardiac diagnosis. However, certain limitation and technical aspects have to be understood in order to apply this valuable tool. Reason for apparent, but erroneous appearance of origin of left coronary artery in both patients is due to “drop-out” artifact. Only a thin tissue separates the coronary artery and the aorta. The coronary artery runs close to the aortic lumen, but turns towards main pulmonary artery with only a thin membrane of tissue separating the lumen of aorta from the lumen of coronary artery. If this tissue-membrane were to be in the same direction as the ultrasonic waves (Figure 5), there can be a “drop-out” artifact leading to this apparent appearance. However, color Doppler imaging clearly shows reversed direction of flow i.e. flow towards aorta which is hemodynamically impossible. Based on clinical suspicion and color Doppler imaging, angiography was performed. The diagnosis was established. These two cases demonstrate the importance of familiarity of the physics of ultrasonography and importance of using color Doppler imaging in conjunction with 2-dimentsional imaging in the evaluation of coronary arteries during echocardiography. These two modalities (2D and Color Doppler imaging) should be routinely applied in all children undergoing echocardiography. Case 1: Ten month old baby girl was admitted with history of fast breathing, feeding difficulty, excessive sweating and feeding difficulties for 3 months. There was history of recurrent respiratory symptoms since 3 months of age. There was heart murmur. Chest X-ray showed Cardiomegaly. Echocardiogram was showed dilated left ventricular (LV) and depressed LV systolic function, and severe mitral regurgitation noticed. Of note, left coronary artery appeared to originate apparently from aorta (Figure 1A) by 2-Dimensional image. However. Color Doppler imaging (Figure 1B) showed reversed flow in left coronary artery (flowing towards the aorta, Blue in Figure 1B). This finding prompted coronary angiography. Angiography confirmed anomalous origin of left coronary artery from pulmonary artery (ALCAPA) and not from aorta (Figure 2). 1A: 2D image 1B: Color Doppler image Ao Ao Apparent LCA Origin from Ao. (Drop-out artifact) Figure 1: Panel1A shows drop-out artifact creating an apparent appearance of left coronary artery origin from aorta (thick arrow). Panel 1B shows color Doppler imaging. Blue color indicates reversed direction of flow in left coronary artery (thin arrows) which is abnormal. Early Frame Late Frame Location of Drop-out Artifact RCA only LCA not seen LCA fills late & retrograde Figure 5: Cartoon illustrating the direction of ultrasonic waves, parallel to the tissue separating aortic lumen from coronary artery lumen. Arrow shows the location of “drop-out” artifact. Conclusions Figure 2: Lateral view of aortogram. Left panel is an early frame showing only right coronary artery (RCA) originates from aorta. Right panel (Late frame) shows delayed, retrograde filling of left coroanry artery (LCA) which eventually empties into main pulmonary artery confirming the diagnosis of ALCAPA. ALCAPA is a life-threatening coronary anomaly, These two cases underscore the importance of applying both 2-Dimensional and color Doppler imaging as part of the routine evaluation of coronary arteries in pediatric echocardiography protocols. Detection of these cases were possible due to strict institution of the pediatric echocardiography protocol. Case 2: Fourteen year old boy, presented with exercise-related chest pain and palpitation. During early childhood patient had frequent hospitalizations for croupy episodes. On physical examination a heart murmur was detected. Electrocardiogram showed left axis deviation with left anterior hemi block. 2-Dimentional echocardiogram in this case also (Fig 2A) shows apparent origin of left coronary artery from aorta. But color Doppler imaging shows (Fig 2B) reversed direction of flow towards aorta (arrows, showing blue flow in Figure 2B). This prompted angiography. Angiography confirmed ALCAPA. He underwent uncomplicated surgery and uneventful recovery. References Taylor AJ, Rogan KM, Virmani R: Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 1992;20:640–647. Wesselhoeft H, Fawcett JS, Johnson AL: Anomalous origin of the left coronary from the pulmonary trunk. Its clinical spectrum, pathology, and pathophysiology, based on a review of 140 cases with seven further cases. Circulation 1968;38(2):403–425 George JM, Knowlan DM. Anomalous origin of the left coronary artery from the pulmonary artery in an adult. N Engl J Med 1959;261:993–998. Robinson PJ, Sullivan ID, Kumpeng V, et al: Anomalous origin of the left coronary artery from the pulmonary trunk: Potential for false negative diagnosis with cross sectional echocardiography. Br Heart J 1984;52:272–277. Yang YL, Nanda NC, Wang XF, et al: Echocardiographic diagnosis of anomalous origin of the left coronary artery from the pulmonary artery. Echocardiography 2007;24:405–411. Frommelt MA, Miller E, Willianmson J, et al: Detection of septal coronary collaterals by color flow Doppler mapping is a marker for anomalous origin of a coronary artery from the pulmonary artery. J Am Soc Echocardiogr 2002;15:259–263. 3A: 2D image 3B: Color Doppler image Ao Ao Apparent LCA Origin from Ao. (Drop-out artifact) Figure 2A&B: 2-D (left panel) and color (right panel) Doppler echocardiographic image of the left coronary artery(LCA) showed apparent origin of the LCA from aorta by 2D, but the color flow is abnormal (flow is towards aorta) Texas Pediatric Society Electronic Poster Contest