Download
1 / 41
890 likes | 3.55k Views
Hair and Nail Disorders. Hair. Structure and functions Alopecia Excessive growth of hair Hair pigmentation and hair cosmetics. Structure of hair. Types of hair: 1) Lanugo ( seen in utero ) 2) Vellus 3) Terminal Hair is a keratinized product of hair follicle.

E N D
Hair • Structure and functions • Alopecia • Excessive growth of hair • Hair pigmentation and hair cosmetics
Structure of hair Types of hair: 1) Lanugo( seen in utero) 2) Vellus 3) Terminal • Hair is a keratinized product of hair follicle. It is present all over skin except on vermillion of lips, palms, soles and skin of nail folds.
Functions of hair • Concerned with sexual and social communication • Protective role eg. nasal and eyelash hair • Sensory function: touch sensation
Hair Cycle • Hair follicles undergo a repetitive sequence of growth and rest called the hair cycle. • Period of active hair growth is Anagen. Duration of this phase decides the length of hair. In humans, it is maximum on scalp. • Catagen is the regressive phase in which the follicular activity declines and ceases. • The hair stays in the Telogen (resting) phase till the beginning of next anagen phase.
Disorders of hair Disorders of hair can either be due to : • loss of hair from hair bearing areas (alopecia) • Excessive hair Androgen dependent hair patterns of typically terminal hair (hirsutism) Patterns of increased hair growth other than in androgenic distribution (hypertrichosis)
Alopecia Can be classified as : 1) Non-cicatricial: preservation of follicles on clinical and histologic examination. Common causes are alopecia areata, androgenetic alopecia, female patterned hair loss and telogen effluvium. 2) Cicatricial (scarring): destruction of follicles due to conditions eg: trauma, infections, cutaneous lupus erythematosus, lichen planus. It is irreversible There can be either diffuse or localised (patterned / non-patterned ) hair loss.
Alopecia areata Can be classified as : • Chronic inflammatory disease probably due to a T-cell mediated response in genetically predisposed individuals. Environmental factors may trigger the condition. • Affects any hair bearing area; can be localized, extensive or diffuse. The involvement of all scalp hair is alopecia totalisand all body hair is alopecia universalis. • Associated with atopy, Down’s syndrome, vitiligo, pernicious anemia, myxoedema, diabetes or hypertension in the family.
Alopecia areata • The affected area shows total hair loss without any inflammation; sometimes with short, easily extractable ‘exclamation-mark’ hair at margin. • Grey hair spared (going white overnight). • Regrowth either spontaneous or following treatment; at first fine and unpigmented but later resumes normal colour and calibre • Nail pitting, onycholysis may be associated
Differential diagnosis • Tineacapitis • Trichotillomania • Secondary syphilis • Androgenetic alopecia
Treatment • Majority of cases have spontaneous regrowth of hair without any treatment. • Steroids (usually topical or intra- lesional) • Topical minoxidil • Topical anthralin, phenol • Topical immunotherapy: Dinitrochlorobenzene (DNCB), squaric acid dibutyl ester (SADBE), diphencyprone (DPCP) • Immunomodulators : Cyclosporin • Photochemotherapy
Prognosis Majority will get complete regrowth sometimes without treatment in 1 year. A small percentage end up with severe chronic form. • Poor prognostic indicators : Onset in childhood, atopy, positive family history, extensive involvement , nail dystrophy, other auto-immune conditions.
Androgenetic alopecia (AGA) • Most common cause of hair loss • Male patterned baldness(MPB) : 50% men affected by the age of 50 years • Female patterned hair loss(FPHL): 20-50% women affected by age of 50 years • Most likely inherited as autosomal dominant/ polygenic trait from either parent
Pathogenesis • Hormonal factors- Type 5 alfareductase changes testosterone to dihydrotestosterone (5-DHT). 5DHT facilitates miniaturization of hair. Aromatase in contrast inhibits process of miniaturization. • Androgen receptors may be increased or may be hyper-responsive in areas affected by AGA
Clinical features • Pigmented terminal hairs are progressively replaced by finer, short and virtually non-pigmented hairs. • MPB: pattern of progression is uniform; starts as frontoparietal recession and involves the entire scalp sparing the occipital fringe; graded into 8 stages by Hamilton. • FPHL: widened central parting earliest sign; progresses through 3 stages of Ludwig.
Treatment • Medical : Topical Minoxidil (2 to 10%) Oral Finasteride (1 to 2.5 mg) • Surgical : Follicular unit transplant Scalp reduction • Cosmetic cover : wigs, hair bonding, hair weaving
Telogen effluvium (TE) • Sudden significant hair loss 2-3 months after an offending insult where hair follicles are pushed prematurely from anagen to telogen phase. • Offending insults: fever, post partum, crash dieting, hypoproteinemia, iron deficiency, major surgeries, prolonged anaesthesia, hypo and hyperthyroidism, major internal disease, acute psychologic stress and medication.
Trichotillomania • Psychiatric disorder in which there is a compulsive habit of pulling out the hair. • Bizarre pattern of hair loss in which hair is twisted and broken at various distances from clinically normal scalp • Management: may vary from identification of stressful episode with accompanying support, parent education, support of psychologist and psychiatrist, drug therapy (antidepressants etc.)
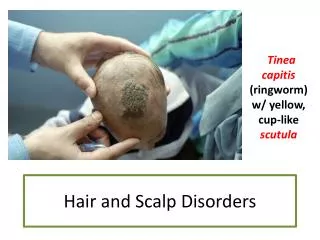
Alopecia due to tinea capitis • Seen essentially in prepubertal age group • It is patchy, incomplete and is due to breakage of hair shaft invaded by dermatophytes. • It is fully reversible except in cases of inflammatory involvement due to species of dermatophytes accidently derived from animals/soil.
Cicatricial alopecia • Seen as an area of thin, shiny, dry and depressed skin with telangiectasia; absence of follicular openings. • Could be developmental/ hereditary, traumatic, secondary to tineacapitis, discoid lupus erythematosus, herpes zoster, bacterial infections, neoplastic disorders, cicatricialpemphigoid, pseudopelade of Brocq • Excision and primary closure for small patches, autografting and scalp expansion, cosmetic camouflage for large patches.
Excessive hair • Growth of hair that in any given site is coarser, longer or profuse than is normal for the age, sex and race • Hirsutism: androgen dependent hair patterns of typically terminal hair • Hypertrichosis: patterns of increased hair growth involving non-androgen dependent follicles
Hirsutism • Growth in female of coarse terminal hair in adult male pattern of distribution i.e. face, chest, upper back • Androgen dependent • Idiopathic or due to hyperplasia / tumors involving ovaries, adrenal cortex or pituitary • May be due to drugs, reduced plasma sex hormone binding globulin, increased androgen receptor or 5 alfareductase activity in skin • Other causes: HAIR-AN and SAHA syndromes
Approach to a hirsute patient • Enquire about the pattern of hirsutism, alopecia, features of virilisation • Probe into the menstrual history, family history and intake of drugs such as glucocorticoids, anabolic steroids. • Systemic examination: Deepening of voice, muscle bulk, loss of body contours, hypertension, striaedistensae and clitoromegaly • Cutaneous examination: Associated acne, acanthosisnigricans, androgenetic alopecia • Investigate to rule out hormonal aberrations like polycystic ovarian or androgen secreting tumors
Treatment • Cosmetic: depilatory creams, plucking, bleaching, electrolysis, eflornithine • Lasers: Nd:YAG, intense pulse light, diode, alexandrite • Hormonal correction: any tumors have to be removed • Drugs: cyproterone acetate, finasteride, flutamide, spironolactone, leuprolide, ketoconazole, medroxyprogesterone acetate
Hair pigmentation and cosmetics • Canities : greying of hair with age • Preamturecanities: onset of greying before 20 years in whites and 30 years in blacks • Poliosis : localised patch of grey hair; congenital and acquired • Hair cosmetics : shampoos, conditioners, hair dyes and bleaches
Nails • Structure and functions • Nail changes in systemic diseases • Nail changes due to systemic drugs • Common skin diseases involving nails • Basic procedures and surgeries
Functions of nails • Help to grasp and manipulate objects • Help in ‘pincer grip’ • Protect terminal phalanx and fingertip • Serve an aesthetic and cosmetic purpose
Nail changes in systemic diseases • Clubbing • Koilonychia • Beau’s lines • Subungual hematoma / Splinter hemorrhages • Color changes of nails • Periungual / subungual tumors
Clubbing 3 major categories: • Idiopathic • Hereditary - congenital • Acquired: • 80% cases associated with respiratory ailments, 10-15% with cardiovascular and the rest with various extrathoracic diseases.
Koilonychia (spoon nails) 3 types: • Idiopathic • Hereditary • Acquired : • Trauma, dermatologic diseases, • Raynaud’s phenomenon, iron deficiency (not the most common cause)
Beau’s lines • Transverse depression across nail plate • Caused by serious systemic illness, drug reaction, bullousdermatoses, severe psychologic stress, local trauma, eczemas, idiopathic
Nail changes due to systemic drugs • Asymptomatic growth rate change and pigmentation abnormalities are the most common changes. • Other changes: Transient shedding, photo- onycholysis, brittle nails, Beau’s lines, permanent nail deformities. • Common drugs: Antibiotics like tetracycline, cephalosporins; fluoroquinolones, antimalarials, retinoids, psoralens, chemotherapeutic drugs.
Common skin conditions with nail changes • Psoriasis • Lichen planus • Fungal infections • Bacterial infections • Viral infections • Ingrown nails (trauma induced)
Nail psoriasis • Seen in upto 50% of patients with psoriasis • May be the first manifestation of psoriasis • Seen in several nails; both finger and toe nails may be affected • Diagnostic signs include extensive irregular pitting, oil drop sign and onycholysis with erythematous borders. • Other abnormalities often seen are nail thickening, subungual hyperkeratosis, nail crumbling etc.
Nail Lichen planus • Nail abnormalities evident in 10% cases with skin / mucosal lichen planus • Commonly occurs in absence of skin / mucosal involvement • Thinning and longitudinal ridging / fisssuring of nail plate, pterygium formation, subungual hyperkeratosis • Permanent destruction may occur
Onychomycosis • Involvement of one / few nails • Examination of skin may give a clue • Four patterns of onychomycosis • Distal and lateral subungualonychomycosis (DLSO) • Proximal subungualonychomycosis (PSO) • White superficial onychomycosis (WSO) • Total dystrophic onychomycosis (TDO)
Onychomycosis: causes • Caused by dermatophytes , candida and moulds • Is known to affect >10% of population in western world • Predisposing factors: occlusive footwear, diabetes mellitus, hyperhidrosis, immunosuppresion, trauma, poor peripheral circulation • Most common pathogens are Trichophytonrubrum, Trichophytonmentagrophytesand candida
Ingrown nail • Common condition due to piercing of nail plate into lateral nail fold • Most common causes are improper trimming of nails and tight, ill-fitting footwear • Great toe nail most commonly involved • Causes inflammation, pain and sometimes formation of extra granulation tissue
Useful investigations • KOH mount • Mycologic culture • Nail clipping • Biopsy-nail plate/nail bed • Radiologic studies
Some therapeutic procedures • Chemical nail avulsion using 40% urea • Nail avulsion: partial and total • Nail splinting • Nail matrix injections • Nail unit biopsy • Chemical/surgical matricectomy • Electrosurgery / radiosurgery / cryotherapy, laser ablation of growths like verrucae, myxoid cyst • Surgical removal of growths like glomus tumor